Posts Tagged memory
[WEB] Is TBI a Chronic Condition?
Posted by Kostas Pantremenos in TBI on January 21, 2024

People with traumatic brain injury (TBI) may continue to improve or decline years after their injury, making it a more chronic illness, according to a study published in Neurology, the medical journal of the American Academy of Neurology.
“Our results dispute the notion that TBI is a one-time event with a stagnant outcome after a short period of recovery,” says study author Benjamin L. Brett, PhD, of the Medical College of Wisconsin in Milwaukee. “Rather, people with TBI continue to show improvement and decline across a range of areas including their ability to function and their thinking skills.”
The study involved people at 18 level 1 trauma center hospitals with an average age of 41. A total of 917 people had mild TBI and 193 people had moderate to severe TBI. They were matched to 154 people with orthopedic injuries but no head injuries. Participants were followed for up to seven years.
Participants took three tests on thinking, memory, mental health, and ability to function with daily activities annually from two to seven years post-injury. They also completed an interview on their abilities and symptoms, including headache, fatigue, and sleep disturbances.
When researchers looked at all test scores combined, 21% of people with mild TBI experienced decline, compared to 26% of people with moderate to severe TBI and 15% of people with orthopedic injuries with no head injury.
Among the three tests, researchers saw the most decline over the years in the ability to function with daily activities. On average, over the course of 2 to 7 years post-injury, a total of 29% of those with mild TBI declined in their abilities and 23% of those with moderate to severe TBI.
Yet some people showed improvement in the same area, with 22% of those with mild TBI improving over time and 36% of those with moderate to severe TBI.
“These findings point out the need to recognize TBI as a chronic condition in order to establish adequate care that supports the evolving needs of people with this condition,” Brett says. “This type of care should place a greater emphasis on helping people who have shown improvement continue to improve and implementing greater levels of support for those who have shown decline.”
A limitation of the study was that all participants were seen at a level 1 trauma center hospital within 24 hours of their injury, so the findings may not apply to other populations.
The study was funded by the National Institute of Neurological Disorders and Stroke, National Institute on Aging, the National Football League Scientific Advisory Board and the U.S. Department of Defense.
[VIDEO] Tips to improve memory
Posted by Kostas Pantremenos in Video on September 15, 2023

Marissa Russell, MS, CCC-SLP | Dementia, Alzheimer’s
Memory is the term given to the structures and processes in our brains involved in the storage and subsequent retrieval of information – and it’s essential to our lives.
However, there are many reasons that our memory may not seem what it was before. Issues may be observed after stroke, brain injury, or a diagnosis of Alzheimer’s, dementia, Parkinson’s, or Mild Cognitive Impairment, or even as a result of normal aging. And while it can be very frustrating, there are some science-based strategies that can help improve memory. In this 5 minute video, Constant Therapy clinician, Marissa Russell, MS, CCC-SLP, walks us through some simple techniques you can use to improve memory.
Watch the video now.
[BLOG POST] Processing Traumatic Memories
Posted by Kostas Pantremenos in REHABILITATION, TBI on April 3, 2023
A friend sent pictures of a camping trip we had gone to when I was approximately 6 months into brain injury recovery following encephalitis. She sounded really excited in her text. To her, they were fond memories and memories she cherished. To me, those encoded memories were painful, traumatic and a reminder of hard times.
The camping trip
At the time we made the decision to join in on a camping adventure, we thought that the change of scenery could do me some good. Although I was still working out what I could and couldn’t do, I had made progress and thought that this undertaking would be ok. In hindsight, I think that I was still very much in denial in terms of what would realistically suit the stage of my recovery. I still didn’t accept my new modus operandi and being the overachiever that I am, I thought that I could still do it all…or at least I was trying very hard to.
I wasn’t too sure how to approach her text. I didn’t want to taint her own memories, but at the same time, I felt it was important to acknowledge how I recalled those memories from the camping trip. Looking at the pictures instantly brought a wave of sadness and I had to take a few deep breathes to avoid seeing tears roll down my cheeks. How could photos bring up such opposite emotions? For one, it is a reminder of a fun time, yet for me, looking at the pictures made me feel sick to my stomach…luckily not as sick as I had felt back then.
It also brought on a wave of guilt. Guilt at the thought of having been so foolish to think that I could have handled such a trip at that particular time of my brain injury recovery. Camping implies prepping a whole lot of stuff ahead of the trip, sleeping on an air mattress, struggling to fall asleep in a tent for afternoon naps, being out and about all day with the kids, having lots of chats with the camping mates, nights games and so much more. In the best of times, this would have been a fun adventure, but I remember feeling completely and utterly exhausted by the time we had finished setting up the tent. It was simply way too much stimulation for my recovering brain.
By then, all my symptoms were on high alert, my brain battery was nearing critical levels and I was feeling so so green.
I attempted to join in on a few activities, only to see Greg having to double track and bring me back to our campsite for a rest. I was sad and frustrated at the thought of seeing everyone else sharing good times and making memories with family and friends, while I, could simply not partake. In lots of ways, I couldn’t fathom how camping could have such a huge flow on effect on my health. On the other hand, I wondered whether the others realised and appreciated how much of a toll the camping trip was taking on my health.

Coming to term with my new reality
I was physically and emotionally drained. I tried so hard to save face, but inside, there was a range of emotions brewing. I felt like I could have either snapped or burst into tears at any moment. The camping trip made me realise that life was now very different. It made me aware of my limitations and there was no denying or hiding them anymore. While out camping, I couldn’t hide in my room or pretend for a short amount of time either. It was there on display for everyone to see and I remember feeling very vulnerable about this.
I didn’t want special treatment, but I couldn’t carry on or survive the next few days without special treatment either…for someone so fiercely independent, it was heart crushing. I was supposed to be the strong one, and back then, I had not realised that strength came in different shapes and sizes.
The trip eventually came to an end. I had survived, but just! It took weeks for me to recover and the state of my mental health had taken a turn for the worst. There was lots to process and I had no idea where to start. Do I deal with the physical symptoms first, do I try to let go of the sadness, frustrations and anger, do I try to grieve, do I work on acceptance? Truth is, I probably had to do all of the above but I had energy for none of those. Survival mode prevailed.
How do I look at it now?
I think that in a weird wonderful way, the pictures sent by my friend have given me the opportunity to revisit and reprocess such painful and sad memories. I don’t think I had realised how painful those stored memories were for me until I got to see them 5 years on. Being in survival mode, I probably subconsciously blocked those memories back then and their associated emotions. Just like there was no hiding during that particular camping trip, I couldn’t ignore the emotions that the pictures brought back to the surface.
I’ve given so much thought about this particular phase of my life this week. I guess the beauty of being further ahead in recovery is that I now know that I can’t change what happened on the camping trip, I can’t change how I have or haven’t handled certain aspects of my recovery back then, but I can try to deal and re-frame those memories and emotions that may have been left in shamble. In good old fashion, writing has been a useful exercise for me to do that.
I know that I have come a long way since that camping trip and I am grateful to be in the position that I am now. Maybe the camping trip will always be associated with a hard phase of my life because it actually was a very hard phase of my life. I am hoping that re-visiting those memories and emotions is a piece of the puzzle that will go towards further healing and grieving from this big life changing event that occurred in August 2017. I am hoping that next time that I retrieve those memories that they aren’t as synonymous of pain as what they were this week.
As painful as it was to look at those memories a few days ago, I am now glad to have been put in this position. They say that growth occurs in the most unlikely places and when we least expect it, I like to think that there is some truth to this.
How have you approached the reminders of painful memories? Have you tried to re-process and encode those memories differently?
[WEB] Memory Motivation
Posted by Kostas Pantremenos in Cognitive Rehabilitation on December 19, 2022

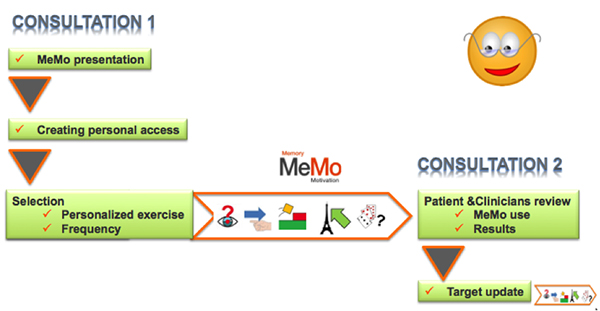
MeMo was designed to respond to the needs of patients with cognitive impairment, of healthcare professionals working on the prevention of cognitive decline, cognitive training and stimulation, as well as of any person willing to train his/her memory and concentration.
MeMo is adapted to patients with the following pathologies:
- Alzheimer’s disease and related disorders
- Traumatic brain injury
- Stroke
- Multiple sclerosis
- Epilepsy
MeMo is the expansion of the work the Innovation Alzheimer association, CoBTeK University of Nice Sophia Antipolis research team working directly with patients from the Nice memory Center, as it provides them with additional ICT-based materials to stimulate and train memory, attention, executive functions, language and gnosis.
MeMo can indeed be employed by clinicians with their patients in individual or group sessions and by the patients alone at home, as a continuation of the work done with the therapist. Till July 2015, MeMo games were regularly proposed to the patients at the Nice Memory Center.
MeMo is freely available on the internet, and can be used on any pc/laptop or tablet.
The exercises are designed and developed by neuropsychologists, medical doctors, researchers and engineers. Every exercise was conceived to train a specific cognitive function, to allow a personalized training based on the observed deficit.
MeMo also allows keeping track of the evolution of performance overtime. After creating an account, the user can track the evolution of his/her performance in the exercises, which can boost motivation and valorize the efforts. This also allows the therapist to follow the evolution of patient’s performance over time.
Our aim is to adapt MeMo and its exercises to the users, by seeking an optimal ease of use. Our team is working continuously to add new games, fix problems and make improvements to the website and the exercises.
Copyright © 2014 – emedinovo
[PDF] Enabling self-management following stroke: A checklist for patients, families, and caregivers
Posted by Kostas Pantremenos in Caregivers on December 4, 2022

Introduction
Heart & Stroke is committed to supporting people who have experienced a heart condition, stroke,
and vascular cognitive impairment. People with these conditions, their family members, and
caregivers, demonstrate incredible resilience as they find ways to adapt and manage living with
these conditions. Teaching self-management skills and providing timely information and education
are key components of success for people with lived experience across the full continuum of care.
This checklist is designed to support those who are transitioning home after a stay in hospital by
offering guidance to people recovering from stroke and their families and caregivers.
It provides tips to help guide recovery after stroke while aligning to Canadian Stroke Best Practice
Recommendations. People are encouraged to use this list to discuss different aspects of recovery
with their stroke care team.
Recovery is a process that can last months and even years after a stroke. It is important to
challenge your body every day, but to do so safely and remember that everyone’s recovery is
different. The tips listed here are a starting point to support your journey. It is important to also
check back regularly with your therapists for additional support as needed.
For more information and strategies to support your recovery, please View PDF
[BLOG POST] 7 principles of neuroscience every coach and therapist should know
Posted by Kostas Pantremenos in Neuroplasticity on December 3, 2022
What does neuroscience have to do with coaching and therapy?
Short answer: Quite a lot!
If you’re a coach or therapist, your job is to facilitate change in your client’s
- thinking (beliefs and attitudes)
- emotions (more mindfulness and resilience)
- behaviour (new healthy habits).
Coaching builds the mental skills needed to support lasting change. Skills such as:
- mindfulness
- self-awareness
- motivation
- resilience
- optimism
- critical thinking
- stress management
Health and wellness coaching, in particular, are emerging as powerful interventions to help people initiate and maintain sustainable change.
And we have academic research to support this claim: check out a list of RCTs in table 2 of this paper).
How can neuroscience more deeply inform coaching and therapy?
Back in the mid-1990s when I was an undergrad, the core text of my neuroscience curriculum was ‘Principles of Neural Science’ by Eric Kandel, James Schwartz and Thomas Jessell. Kandel won the 2000 Nobel Prize in Physiology or Medicine for his research on memory storage in neurons.
A few years before his Nobel, Kandel wrote a paper ‘A new intellectual framework for psychiatry’. The paper explained how neuroscience can provide a new view of mental health and wellbeing.
Based on Kandel’s paper, researchers at the Yale School of Medicine proposed seven principles of brain-based therapy for psychiatrists, psychologists and therapists. The principles have been translated into practical applications for health & wellness, business, and life coaches.
One fundamental principle is,
“All mental processes, even the most complex psychological processes, derive from the operation of the brain.”
And another is:
“Insofar as psychotherapy or counseling is effective . . . it presumably does so through learning, by producing changes in gene expression that alter the strength of synaptic connections.”
That is, human interactions and experience influence how the brain works.
This concept of brain change is now well established in neuroscience and is often referred to as neuroplasticity. Ample neuroscience research supports the idea that our brains remain adaptable (or plastic) throughout our lifespan.
Here is a summary of Kandel, Cappas and colleagues thoughts on how neuroscience can be applied to therapy and coaching…
Seven principles of neuroscience every coach should know.
1. Both nature and nurture win.
Both genetics and the environment interact in the brain to shape our brains and influence behaviour.
Therapy or coaching can be thought of as a strategic and purposeful ‘environmental tool’ to facilitate change and may be an effective means of shaping neural pathways.
2. Experiences transform the brain.
The networks of our brain associated with emotions and memories such as the pre-frontal cortex, the amygdala, and the hippocampus are not hard-wired — they are ‘plastic’. The brain prunes and tunes its connections in response to the experiences it has.
3. Memories are imperfect.
Our memories are never a perfect account of what happened. Memories are re-written each time when we recall them depending on how, when and where we retrieve the memory.
For example, a question, photograph or a particular scent can interact with a memory resulting in it being modified as it is recalled.
With increasing life experience we weave narratives into their memories. Autobiographical memories that tell the story of our lives are always undergoing revision precisely because our sense of self is too.
Consciously or not, we use imagination to reinvent our past, and with it, our present and future.
4. Emotion underlies memory formation.
Memories and emotions are interconnected neural processes.
The amygdala, which plays a role in emotional arousal, mediate neurotransmitters essential for memory consolidation. Emotional arousal has the capacity to activate the amygdala, which in turn modulates the storage of memory.
Research suggests each of us constructs emotions from a diversity of sources: our physiological state, by our reactions to the ‘outside’ environment, experiences and learning, and our culture and upbringing.
5. Relationships are the foundation for change
Relationships in childhood AND adulthood have the power to elicit positive change.
Sometimes it takes the love, care or attention of just one person to help another change for the better.
The therapeutic relationship has the capacity to help clients modify neural systems and enhance emotional regulation.
6. Imagining and doing are pretty much the same thing to the brain.
Mental imagery or visualisation not only activates the same brain regions as the actual behaviour but also can speed up the learning of a new skill.
Envisioning a different life may as successfully invoke change as the actual experience.
7. We don’t always know what our brain is ‘thinking’.
Unconscious processes exert great influence on our thoughts, feelings, and actions (but I’m not willing to put a percentage on ‘how much is subconscious’).
The brain can process nonverbal and unconscious information, and such information influences therapeutic and other relationships. It’s possible to react to unconscious perceptions without consciously understanding the reaction.
[WEB] What is a Neuropsychologist?
Posted by Kostas Pantremenos in Educational on November 29, 2022

A neuropsychologist is someone who can assess people who are having problems with memory, thinking, or concentration or who have experienced changes in personality, behavior, awareness, or language. Neuropsychologists—who have doctoral degrees in psychology and specialized training in neuroscience and nervous system disorders such as dementia, stroke, and epilepsy— administer standardized cognitive and behavioral tests to better determine patients’ levels of difficulty.
In addition to performing tests, neuropsychologists conduct thorough examinations, including reviews of symptoms and medications and interviews with patients and sometimes family members, who may provide more detailed descriptions of any changes they’ve observed in the patients.
During typical cognitive tests, a patient may be asked to review lists of words that the neuropsychologist will ask them to repeat at different points during visits. For another test, a patient studies a design on a piece of paper and re-creates it using colored blocks. Each test assesses memory or other cognitive functions such as reasoning, language, or visuospatial abilities. The neuropsychologist tries to identify patterns that point to different brain disorders. The interviews, the test results, and the history of the patient’s symptoms help a neuropsychologist determine if the patient’s responses are normal for his or her age, identify key abnormalities, and consider which disorder may be causing the disturbance.
Evaluations usually employ a set battery of tests. Additional questions are tailored to each person, based on education, occupation, and past experiences. For example, a memory test for someone with a graduate degree and a technical job might involve remembering a list of 15 words. For someone with a high school diploma and a job in the service industry, it might be a list of 10 words. This allows the neuropsychologist to detect patterns on a simpler test that might be missed on a harder test if it was beyond the scope of the patient’s experience.
During the examination, the neuropsychologist may measure reaction time to questions and consistency of answers to provide a fuller picture of the situation and to make recommendations for care, if needed. As the specialty has grown, neuropsychologists have begun seeing patients at earlier stages, which allows patients and families to plan for the future and start treatments sooner.
Patients may need just one visit, which can last two to six hours, depending on the questions asked and level of the patients’ function. After the examination, the neuropsychologist’s assessments and recommendations are sent to the patient’s doctor or neurologist. Recommendations may include referrals to occupational or speech therapists, brain scans, driving evaluations, and tips for making the patient’s house less cluttered and confusing. Neuropsychologists also may provide referrals to support groups and counseling for caregivers.
The neuropsychologist may ask a patient to come back with a family member for a follow-up visit. If a patient has a progressive disorder, the neuropsychologist may schedule a later visit to assess any changes and make new recommendations.
Neuropsychologists may be part of a neurology or gerontology practice or may be in private practice. They also may work with neuropsychiatrists—psychiatrists who focus on behavioral illnesses related to brain disorders. Subscribe to Our Email Newsletter!Subscribe Now
Not all insurance companies cover visits with neuropsychologists. Patients and families should check with their insurance providers. Medicare may pay some of the cost, and additional fees may be covered by supplemental insurance.
Dr. Weintraub is a neuropsychologist and professor of psychiatry and behavioral sciences at the Feinberg School of Medicine at Northwestern University in Chicago.
[WEB] How Does Epilepsy Affect Memory?
Posted by Kostas Pantremenos in Epilepsy on August 12, 2022

People with epilepsy, a condition characterized by seizures (also known as convulsions), commonly experience changes in memory and cognition. Cognition is the process of thinking, reasoning, and remembering.
One type of epilepsy in particular, called temporal lobe epilepsy, has been linked to memory loss due to its effects on a brain structure called the hippocampus. The type of memory loss may vary. For example, people may forget about appointments or taking medication. Others may remember the distant past but have trouble remembering what happened last week.
So how, exactly, does epilepsy affect memory, and is there anything people can do about it?
What Types of Seizures Affect Memory?
Temporal lobe seizures are most closely associated with memory loss or cognition problems. This is because the temporal lobe is the home of the hippocampus, the part of the brain responsible for creating and storing new memories. However, according to the Epilepsy Society, any type of seizure has the potential to cause memory problems. If a person tends to have focal seizures (seizures that only affect part of the brain), the effect of the seizures will vary depending on where in the brain the seizures happen. If these focal seizures do not originate in or near the hippocampus, they have less of a chance of affecting memory. The frontal lobe is also important for memory, and damage to this area may result in memory impairment.
Generalized seizures, which affect both halves (or hemispheres) of the brain, can also affect memory. According to the Epilepsy Foundation, individuals who have mostly primary generalized seizures (such as absence, myoclonic, or tonic-clonic seizures) are less likely to have memory issues than those who have partial seizures (especially where the frontal or temporal lobes are involved).
The Hippocampus and Memory
The hippocampus is a small curved structure of the brain that lies deep inside the temporal lobe (the part of the brain on either side of the head, behind the ears). It is responsible for certain types of memory and learning. Specifically, the hippocampus transforms short-term memories into long-term memories. This process is called memory consolidation. Seizures that start in the hippocampus (or spread to it) can cause problems with memory.
The hippocampus also helps with remembering (a process known as memory recall or retrieval). When a person tries to recall certain types of memory, the hippocampus helps to retrieve the information from the brain’s cortex to enter it into an active state in the person’s mind. This is why damage to this region can potentially impair the details of past memories.
Because seizures can permanently affect the cells in the hippocampus, memory loss can become permanent.
Declarative Memory and Epilepsy
The memories most frequently affected by seizures are declarative memories. Declarative memories are of particular facts or events. These are further broken down into episodic memories (events from a person’s life) and semantic memories (facts or general knowledge). Research has shown that only episodic memory is affected by temporal lobe epilepsy and semantic memory is not. People will be more likely to forget events from their past but will be more likely to remember general information about the world. Verbal memory deficits in a laboratory setting have also been noted in individuals with epilepsy. Children with epilepsy are also susceptible to memory deficits.
Epilepsy Medications and Memory
Medications people take for epilepsy — antiepileptic drugs or antiseizure medications — can also cause memory problems. Many people experience drowsiness when on antiepileptic drugs. This causes concentration problems that affect short-term memory and make it more difficult to learn new information. If you are concerned about how your medication is affecting your memory, you should talk to your doctor. However, never discontinue taking medication without consulting your doctor first.
How Do Memory Problems Affect People’s Lives?
Memory problems can seriously affect the day-to-day well-being of people living with epilepsy, as well as decrease their quality of life. This is why early and efficient seizure control through medications is critical in order to preserve memory as much as possible.
According to the Epilepsy Foundation, there are two approaches people with epilepsy can take to improve their memory. One is an indirect approach, through which people improve their memory by focusing on factors such as seizure control. The second is a direct approach, through which people treat their memory problems with medication (such as stimulants) or with strategies to change behaviors and improve memory recall.
Strategies To Improve Memory
People with epilepsy may wonder if there is anything they can do to help them improve their memory or remember things. One strategy recommended by a member of MyEpilepsyTeam is to write down important information after having a conversation with someone.
One study showed that a memory-rehabilitation or memory-training program can help individuals with epilepsy who struggle with memory problems. Another study found that the drug memantine helped improve memory outcomes in people with focal epilepsy. These effects could also have been due to practice by the study participants, and these results should be interpreted cautiously.
Surgery for epilepsy has also been shown to have varied impacts on epilepsy-related memory problems. For instance, one study found that children with temporal lobe epilepsy who had temporal lobe surgery had mixed results when it came to their memory tests. Specifically, the study found that surgery improved attention or working memory scores, some verbal episodic memory tasks, and naming-test performances. However, children with left temporal lobe epilepsy had worse verbal memory results, and children with right temporal lobe epilepsy had worse visual memory results.
Memory improvement strategies for people with epilepsy are also possible through working with allied health professionals like occupational therapists, physiotherapists, and speech-language pathologists. They can help people learn recall strategies and memory compensatory behaviors, and they can help mitigate some of the other neurologic effects of epilepsy.
What Are People With Epilepsy Saying About Memory?
People on MyEpilepsyTeam sometimes discuss their experiences with epilepsy and memory problems. For instance, one member wrote, “It seems like most of my memory loss started in the last three years.” Another member asked, “Since having epilepsy, do you have trouble remembering things?” They further elaborated, “Each time I have a seizure, it’s like more and more of my memory is taken.” However, another member said that memory does come back, to some extent.
In another daily post, a member explained that they are, “Still recovering from five seizures I had a week ago. Still having trouble remembering everything.” Another member wrote, “I’m so tired of not remembering.”
Memory loss is common in people with epilepsy, and it’s frustrating. Finding a community of people who are experiencing the same things you are going through may help you cope.
Building a Community
MyEpilepsyTeam is the social network for people with epilepsy. On MyEpilepsyTeam, more than 99,000 members come together to ask questions, give advice, and share their stories with others who understand life with epilepsy.
Are you living with epilepsy? Share your experience in the comments below, or start a conversation by posting on MyEpilepsyTeam.
[Abstract] Comparison of cognitive rehabilitation efficacy based on Computer-Assisted Cognitive Rehabilitation with and without transcranial direct current stimulation (tDCS) on improving the working memory of stroke patients.
Posted by Kostas Pantremenos in Cognitive Rehabilitation on June 12, 2022
Abstract
Introduction: Working memory deficit is one of the most common complaints in post-stroke patients. The present study aimed to investigate the efficacy of the con-commitment use of unihemispheric concurrent dual-site a-tDCS (a-tDCSUHCDS), computer-assisted cognitive rehabilitation and conventional (Single site) a-tDCS in comparison with computer-assisted cognitive rehabilitation without tDCS on the working memory in stroke patients.
Method:32 participants (21 males and11 females; age range 40-65years) with subacute stroke were selected by purposeful sampling method & randomly assigned to three experimental conditions and a controlled group with sham stimulation. All groups completed sessions of the Dual N-back training task. A-tDCSUHCDS group received anodal tDCS over the left DLPFC and M1 and conventional (Single site) a-tDCS group received anodal tDCS over the left DLPFC.
Result: A repeated measures analysis of variance revealed that the a-tDCSUHCDS group had the larger improvement in working memory tasks after the intervention. Also, at the 8-weeks follow-up, the a-tDCSUHCDS group still had larger improvements in mentioned tasks.
Conclusion: These results indicated that there may be potential for the concomitant use of a-tDCSUHCDS and computer-assisted cognitive rehabilitation by increasing the excitability of the cortical network of brain regions that play an important role in executive functions, to enhance the efficiency of the cognitive rehabilitation programs of the stroke patients.
[WEB] Is Lumosity a Lie? The Neuroscience Behind Brain Training Games
Posted by Kostas Pantremenos in Video Games/Exergames on April 20, 2022

Brain training games promise to improve your memory, prevent cognitive losses and decrease your chances of showing symptoms of dementia – are their promises too good to be true?
Video games have become so much more than a way to pass time – they’re used as simulations for teaching and training, tests of attention and skill, and even as diagnostic tools.
Recently, many online cognitive training platforms such as Lumosity have claimed that their “brain training” video games can help to slow symptoms of neurodegenerative diseases like Alzheimer’s disease, which currently have no cure. Unfortunately, the reality is a little more complicated than Lumosity’s advertisements would suggest.
https://www.youtube.com/watch?v=WfIbIsVRDcM[/embed]
Neuroscience 101
Brain training games base their promises on two theories – the theory of neuroplasticity, and the theory of cognitive reserve.
Neuroplasticity is the process of the brain modifying its pathways as it learns new things. Originally, scientists thought that this process only occurred in childhood, but a breakthrough study by Draganski et al. in 2004 demonstrated that adults learning a new task (in this case, juggling) developed new, longterm physical changes in their brain’s composition.
This breakthrough was huge for neuroscience, because it showed that adults can modify the structure of their brain even after it has matured.
Further studies have shown that these structural changes can even occur in adults diagnosed with Mild Cognitive Impairment — a high risk factor for the development of dementia.
The theory of cognitive reserve goes hand-in-hand with neuroplasticity. This theory proposes that life experiences, cognitive activities, and unique skill sets can allow your brain to compensate for the structural changes that come with aging and dementia by building new pathways.
Essentially, cognitive reserve is the “use it or lose it” theory – the more you use your brain, the more pathways it builds through neuroplasticity, and the longer it will take for you to show symptoms of cognitive decline or dementia.
What do Brain Training Games Look Like?
Brain training games come in all shapes and sizes.
While Lumosity is one of the best known companies in its industry, there are innumerable apps, video games, and websites available that are dedicated to brain training.
There is some variation between companies, but brain training games feature simple controls and design that allow the player to focus on a single cognitive skill such as memory, attention, processing speed, or problem solving. The games increase in difficulty over time.
The games are offered as “training programs” that are intended to be completed daily, and these programs may be individualized to some degree.
Competition in brain training games is usually limited to competition against yourself — trying to improve your score in individual games, or an overall “brain health” score calculated at ongoing intervals which may offer comparisons to others that are of your age and education level.
While the games are simple and are targeted for non-gaming adults, they can be incredibly frustrating — there is no doubt that they require focus and concentration to complete them quickly and accurately, and it can be addicting to watch your score improve while unlocking new levels.
So What is the Problem?

To summarize, thanks to neuroscience, we know two things:
- The brain can change even in adulthood when we learn new skills, and
- The more actively we use our brain, the more we decrease our individual chances of developing symptoms of dementia
And, thanks to the research that has gone into the development of brain training games we know that they:
- Focus on building new skills, and
- Place a priority on challenging your brain with new and targeted tasks.
Looking at these facts, it seems hard to believe that brain training games don’t accomplish everything that they say they can – but unbiased research shows that there are some areas where they definitely don’t measure up.
In fact, the Stanford Centre of Longevity released a statement written by cognitive psychologists and neuroscientists that referred to the claims made by brain training websites as “exaggerated and misleading” — a statement that definitely should not be taken lightly.
“[…] exaggerated and misleading claims exploit the anxiety of adults facing old age for commercial purposes. Perhaps the most pernicious claim, devoid of any scientifically credible evidence, is that brain games prevent or reverse Alzheimer’s disease.”
Where do Brain Training Games Fall Short?

Lumosity boasts that it has 70 million members, many of whom are paying a monthly subscription fee to access their full library of brain training games – a practice shared by most other brain training services.
For this reason, it’s imperative that users understand what they are (and aren’t) getting from the time and money they spend on brain training.
The best way to explain brain training games like Lumosity is that they are essentially an answer key for cognitive tests.
You will definitely improve in your ability to play the brain training games (as you would with any other video game), and your test scores will likely improve (because the brain training games are correlated to questions commonly used in cognitive tests).
However, many unbiased studies have shown that it is unlikely that the time you spend playing brain training games will actually enable you to use your brain in the ways that you want to use it in your daily life.
Essentially, brain training games only train your brain to play the games — they do not train your brain for the problems that it will encounter in real life, and studies agree that it is unlikely that they actually contribute towards your cognitive reserve.
So… Is Lumosity Lying?

Over the past couple of years, Lumosity has toned down a lot of the language that they use concerning their brain training games. They may not be making explicitly false promises, but their insinuations are still pretty misleading.
While their homepage points to scientific studies and PhD’s, it’s important to remember that many of these studies and individuals are funded by Lumosity — greatly increasing the likelihood that a positive end result will be reported.
When all of the literature is examined, there just isn’t the support that Lumosity claims there is. Lumosity’s games are great in theory, but they have failed to demonstrate any incredible positive effects when examined by outside sources.
The Future of Brain Training

The take-away from this article shouldn’t be that video games will never be able to help prevent age-related cognitive decline and memory loss, nor should it be that time spent on Lumosity or similar websites is time wasted.
As we mentioned above, the logic for brain training games is THERE, and there is research to support the general idea of computerized brain training games. However, in its current state we just aren’t quite able to achieve the results that we want.
In fact, a 2014 study by Shute, Ventura and Ke showed that participants who played Portal 2 (a video game that makes use of strategy and puzzles but isn’t focused on cognitive training) was far more effective than Lumosity in improving students’ performance on measures of problem solving, spatial skills, and persistence.
The real truth of the matter is that this is one of the research areas that could change the world – but there is so much more research and innovation required in this area before that can happen.
While Lumosity may not be providing its users with protective gains in cognitive reserve, it is collecting tons of data about how users interact with brain training game and their efficacy (to a point). This data will be invaluable to game designers and neuroscientists moving forwards.
I fully believe that in the future there will be incredible, immersive video games that do allow users to learn new skills, improve their problem solving, and slow cognitive decline – but the research isn’t there to support the brain training platforms that are available right now.
What Should I Do Now to Keep My Brain Healthy?
Go for a walk. Learn a new language. Eat a balanced diet. Meet new people. Take up a new hobby. All of these pastimes are great, scientifically supported, ways to keep your brain active, reduce risk factors of developing dementia, and create cognitive reserve.
If you enjoy the games on Lumosity and the challenges that they offer there is no reason to stop playing the games — it’s just important that you don’t think playing twenty minutes of basic video games five times a week is enough targeted cognitive intervention to truly decrease your risk of developing symptoms of dementia or to improve your overall cognitive abilities outside of your skills in-game.
Improving brain health has been a hot topic in the news lately, so we ask you — Do you have a Lumosity membership? What do you think the future holds for interactions between neuroscience and video games?
Image Credit: Human Brain Sagittal View via. Shutterstock

