
Figure 1. Study flow diagram. Data collection occurred at weeks 1, 6, 9, 15 and 18. Cross-over analysis required data from weeks 1, 6, 9 and 15.
Posted by Kostas Pantremenos in Paretic Hand on June 29, 2017
Background The ability to predict outcome after stroke is clinically important for planning treatment and for stratification in restorative clinical trials. In relation to the upper limbs, the main predictor of outcome is initial severity, with patients who present with mild to moderate impairment regaining about 70% of their initial impairment by 3 months post-stroke. However, in those with severe presentations, this proportional recovery applies in only about half, with the other half experiencing poor recovery. The reasons for this failure to recover are not established although the extent of corticospinal tract damage is suggested to be a contributory factor. In this study, we investigated 30 patients with chronic stroke who had presented with severe upper limb impairment and asked whether it was possible to differentiate those with a subsequent good or poor recovery of the upper limb based solely on a T1-weighted structural brain scan.
Methods A support vector machine approach using voxel-wise lesion likelihood values was used to show that it was possible to classify patients as good or poor recoverers with variable accuracy depending on which brain regions were used to perform the classification.
Results While considering damage within a corticospinal tract mask resulted in 73% classification accuracy, using other (non-corticospinal tract) motor areas provided 87% accuracy, and combining both resulted in 90% accuracy.
Conclusion This proof of concept approach highlights the relative importance of different anatomical structures in supporting post-stroke upper limb motor recovery and points towards methodologies that might be used to stratify patients in future restorative clinical trials.
Stroke is one of the the most common causes of physical disability worldwide and about 80% of stroke survivors experience impairment of movement on one side of the body.1 Hand and arm impairment in particular is often persistent, disabling and a major contributor to reduced quality of life.2 The main predictor of long-term outcome of upper limb function is the level of initial impairment.3 This can be quantified as the proportional recovery rule which states that by 3 months, patients with stroke will recover about 70% of the initial upper limb motor impairment that has been observed on day 3 post-stroke.4–6 The prediction works extremely well for those presenting with mild to moderate upper limb impairment, but in only about half of those with initially severe upper limb impairment.4–6 In the other half, patients do worse than predicted, that is, there is a failure of proportional recovery. A key question then is, what is the difference between patients with stroke matched for initial severity who go on and have different recovery trajectories? The answer to this will point to the factors that are important for the dynamic process of recovery independent from the causes of initial impairment.
One possibility is the anatomy of the damage may be different in each group. A number of recent studies have proposed that the corticospinal tract (CST) plays a decisive role in this categorical difference7–11 as cortical reorganisation for improved motor function ultimately requires access for cortical motor areas to muscles. However, CST lesion load correlates with initial motor impairment,12 which is the major predictor of long-term outcome. It is therefore reasonable to ask how much CST lesion load can improve prediction of long-term outcome over and above initial severity. Furthermore, most of the patients involved in these studies had suffered from subcortical stroke and recent work has suggested that taking account of cortical damage after stroke can improve prediction of the motor clinical consequences.13 14
In this study, we investigated 30 patients with chronic stroke with a range of lesion locations (cortical and/or subcortical involvement) known to have presented with severe initial upper limb impairment but who had gone on to have quite different recovery trajectories. We applied a support vector machine approach to data representing lesion likelihood derived from structural T1-weighted MRI to answer the following questions. First, how accurately can patients with stroke with severe initial upper limb impairment be classified as having either good or poor recovery using only data extracted from whole brain structural MRI? Second, which brain regions contribute most to the classification? The results have the potential to transform how prediction of long-term upper limb outcome after stroke is achieved in routine clinical practice in future. The ability to easily and accurately predict outcome with standard clinical neuroimaging would have important implications for planning of treatment but also for stratification in future trials of restorative therapies.15[…]

Figure 1 Data representation. In the figure to the left, a mask corresponding to the corticospinal tract is overlaid on an image obtained through lesion likelihood. Each voxel corresponds to a value between 0 and 1 encoding the probability of being part of injured tissue. The enlarged section of the image in the figure to the right shows that each voxel within a region of interest corresponds to a particular feature in the multivariate analysis.
Posted by Kostas Pantremenos in Functional Electrical Stimulation (FES) on June 29, 2017
The Christopher & Dana Reeve Foundation’s NeuroRecovery Network® (NRN) nine rehabilitation centers will receive 30 Restorative Therapies’ Xcite electrical stimulation systems.

Xcite multichannel electrical stimulation for neuro re-education
BALTIMORE, MD (PRWEB) JUNE 28, 2017
The Christopher & Dana Reeve Foundation’s NeuroRecovery Network® (NRN) supports cutting-edge Clinical Rehabilitation Centers and Community Fitness and Wellness Facilities (CFWs) that make up two branches of care for people living with spinal cord injury and other physical disabilities.
The nine NRN rehabilitation centers and CFWs will receive 30 Restorative Therapies’ Xcite systems which will be used to implement NRN’s cutting edge NMES rehabilitation program for patients across the US. The acquisition was funded by the Reeve NRN Network and the University of Louisville in conjunction with the rehabilitation centers and CFWs.
NMES is a physical therapy rehabilitation modality used to evoke sensory feedback, functional movements and exercise not otherwise possible for individuals with a neurological impairment such as a spinal cord injury, stroke, multiple sclerosis or cerebral palsy.
The Xcite system delivers up to 12 channels of electrical stimulation to nerves which activate core, leg and arm muscles. Easy to use sequenced stimulation evokes functional movement enabling a patient’s paralyzed or weak muscles to move through dynamic task specific movement patterns.
“Xcite is the first truly practical electrical stimulation rehabilitation system of this kind that I have seen. In addition to combining several valuable neuro-rehabilitation interventions, task-specific electrical stimulation, mass practice and neuromuscular re-education, Xcite is portable and easy enough to use that it could be used in the patient’s home,” said Prof. Susan Harkema of the Kentucky Spinal Cord Injury Research Center, University of Louisville. “In the context of rehabilitation influencing neural plasticity as a means for neural restoration, training in the home is an essential component of progress and I see Xcite as a great tool in achieving this,” concludes Harkema.
“The NRN clinical rehabilitation centers and CFWs played a key role during the development of the Xcite system.” says Andrew Barriskill, CEO of Restorative Therapies. “Xcite is designed to be integrated into the cutting edge therapy programs being developed and utilized by the Reeve Foundation’s NRN while at the same time being easy to use within any physical therapy or occupational therapy.”
About Restorative Therapies
Restorative Therapies is the designer of medical devices providing clinic and in-home restoration therapy. Xcite is the next in the series of FES powered physical therapy systems that started with the company’s hugely successful RT300 FES cycle.
Restorative Therapies mission is to help people with a neurological impairment or in critical care achieve their full recovery potential. Restorative Therapies combines activity-based physical therapy and Functional Electrical Stimulation as a rehabilitation therapy for immobility associated with paralysis such as stroke, multiple sclerosis and spinal cord injury or for patients in critical care.
Restorative Therapies is a privately held company headquartered in Baltimore. To learn more about Restorative Therapies please visit us at http://www.restorative-therapies.com
Posted by Kostas Pantremenos in Paretic Hand, tDCS/rTMS on June 28, 2017
Introduction Dexterity is described as coordinated hand and finger movement for precision tasks. It is essential for day-to-day activities like computer use, writing or buttoning a shirt. Integrity of brain motor networks is crucial to properly execute these fine hand tasks. When these networks are damaged, interventions to enhance recovery are frequently accompanied by unwanted side effects or limited in their effect. Non-invasive brain stimulation (NIBS) are postulated to target affected motor areas and improve hand motor function with few side effects. However, the results across studies vary, and the current literature does not allow us to draw clear conclusions on the use of NIBS to promote hand function recovery. Therefore, we developed a protocol for a systematic review and meta-analysis on the effects of different NIBS technologies on dexterity in diverse populations. This study will potentially help future evidence-based research and guidelines that use these NIBS technologies for recovering hand dexterity.
Methods and analysis This protocol will compare the effects of active versus sham NIBS on precise hand activity. Records will be obtained by searching relevant databases. Included articles will be randomised clinical trials in adults, testing the therapeutic effects of NIBS on continuous dexterity data. Records will be studied for risk of bias. Narrative and quantitative synthesis will be done.
This is a novel systematic review and meta-analysis focusing specifically on dexterity.
We use continuous data not dependent on the evaluator or participant.
This work will potentially help future evidence-based research and guidelines to refine non-invasive brain stimulation.
The hand’s somatotopy is extensively represented in the human motor cortex.1 2 Phylogenetically, this relates to the development of corticomotoneuronal cells that specialise in creating patterns of muscle activity that synergises into highly skilled movements.3 This organised hand-and-finger movement to use objects during a specific task is known as dexterity.4 Evolutionary, dexterity played a pivotal role in human survival and is fundamental to actives of daily living, and hence quality of life.5 6
This precision motor movement relies on integration of information from the cerebral cortex, the spinal cord, several neuromusculoskeletal systems and the external world to coordinate finger force control, finger independence, timing and sequence performance.7 During these tasks, multivoxel pattern decoding shows bilateral primary motor cortex activation (M1), which was responsible for muscle recruitment timing and hand movement coordination.8 9 This is related to motor cortex connectivity through the corpus callosum, to motor regions of the cerebellum and white matter integrity.10–15 Adequate motor output translates into successfully executed tasks, like picking up objects, turning over cards, manipulating cutlery, writing, using computer–hand interfaces like smartphones, playing an instrument and performing many other similarly precise skills.16
These motor tasks are negatively impacted when motor output networks are affected, as seen in stroke or Parkinson’s disease.17 18 Therapeutic interventions that restore these damaged motor networks can be vital to restore fine motor movement after injury occurs. Pharmaceutical approaches often lead to adverse effects such as dyskinesias in Parkinson’s disease. Moreover, even after intensive rehabilitation programmes, only about 5%–20% of patients with stroke fully recover their motor function.19–21 Non-invasive brain stimulation (NIBS) techniques, like transcranial direct current stimulation (tDCS) and repetitive transcranial magnetic stimulation (rTMS), are proposed adjuvant or stand-alone interventions to target these affected areas and improve fine motor function.22 23 Briefly, these NIBS interventions are shown to influence the nervous system’s excitability and modulate long-term plasticity, which may be beneficial to the brain’s recovery of functions after injury.24–27
Fine hand motor ability is not studied as much in previous reviews of NIBS. Specifically, one narrative review focuses on rTMS in affected hand recovery poststroke; however, it does not consider the implications of varying International Classification of Functioning, Disability and Health (ICF) domains, data types and rater dependent outcomes, and its interpretability is limited without quantitative synthesis.28–31 The overarching conclusion was supportive of rTMS for paretic hand recovery, though with limited data to support its regular use, and a pressing need to study individualised patient parameters.28 One meta-analysis had positive and significant results when specifically studying the effects of rTMS on finger coordination and hand function after stroke.32 However, while various meta-analysis, and another systematic review, studied upper-limb movement after NIBS in distinct populations, they did not focus on precise hand function, pooled upper-limb outcomes with hand outcomes and presented mixed results.33–38
Motivated by this gap in the evidence for NIBS in dexterity, we will do a systematic review and meta-analysis of the literature on these brain stimulation technologies using outcomes that focus exactly on manual dexterity. These outcomes will be continuous and not dependent on the participant’s or rater’s observation (ie, they will be measured in seconds, or number of blocks/pegs placed, and not by an individual’s interpretation). They will be comprised of multiple domains as defined by the ICF, providing an appreciation of function rather than only condition or disease.29–31 By focusing on the ICF model, we will be able to study dexterity across a larger sample of studies, NIBS techniques and conditions in order to provide a better understanding of brain stimulation efficacy on hand function in various populations.[…]
Posted by Kostas Pantremenos in Pharmacological, Spasticity on June 28, 2017
Objective: To present practice patterns for phenol neurolysis procedures conducted for spasticity management.
Design: A retrospective review of 185 persons with spasticity who underwent phenol neurolysis procedures (n = 293) at an academic rehabilitation hospital and clinic. Patient demographics, concomitant spasticity treatments, and procedure relevant information were collected.
Results: The cohort included 71.9% males and 61.6% inpatient procedures. Neurological diagnoses included stroke (41.0%), traumatic brain injury (28.6%) and spinal cord injury (24.3%). Musculoskeletal diagnoses included spastic hemiplegia or paresis (51.3%), tetraplegia (38.4) and paraplegia (9.2%). At the time of phenol neurolysis, most patients (77.5%) received concomitant pharmacological treatments for spasticity. Injection guidance modalities included electrical stimulation and ultrasound (69.3%) or ultrasound only (27.3%). A mean of 3.48 ml of phenol were injected per nerve and 10.95 ml of phenol were used per procedure. Most commonly injected nerves included the obturator nerve (35.8%) and sciatic branches to the hamstrings and adductor magnus (27.0%). Post-phenol neurolysis assessment was recorded in 54.9% of encounters, in which 84.5% reported subjective benefit. Post-procedure adverse events included pain (4.0%), swelling and inflammation (2.7%), dysaesthesia (0.7%) and hypotension (0.7%).
Conclusion: Phenol neurolysis is currently used to reduce spasticity for various functional goals, including preventing contractures and improving gait. Depending on the pattern of spasticity displayed, numerous peripheral nerves in the upper and lower extremities can be targeted for treatment with phenol neurolysis. Further research into its role in spasticity management, including studies exploring its cost-effectiveness and pharmacological and side-effects compared with other treatment options are needed.
Characterized by hyperexcitable stretch reflexes that increase muscle tonicity and exaggerate tendon jerks, spasticity is a common motor disorder that follows a variety of central nervous system insults (1). Implicated neurological insults most often include stroke, traumatic brain injury (TBI) or spinal cord injury (SCI). Spasticity is often associated with various complications including joint contractures, muscle shortening and postural deformities (1) that lead to multiple impairments. Early goal-directed spasticity management is instrumental in helping increase the likelihood of good outcomes and limiting complications (1, 2). Unfortunately, a lack of universally standardized management and an abundance of therapeutic options make spasticity management a challenging task.
Currently, spasticity is frequently managed through a combination of therapeutic modalities, pharmaceutical options and surgical procedures (3). Pharmaceutical options include medications delivered orally, via local injections, or through intrathecal pumps. Oral medications, including baclofen and tizanidine, help decrease spasticity (3). However, systemic side-effects, such as generalized muscle weakness, sedation, confusion, and hypotension, preclude the use of higher dosages that might be warranted for control of moderate-to-severe spasticity (3, 4). Intrathecal baclofen pump (ITB) is often indicated in treating severe and/or diffuse spasticity as a means to deliver high-dosage baclofen with less concern for systemic side-effects (4). Although ITB treatment is very effective, numerous complications and the requirement for commitment to maintenance associated with this treatment makes it favourable only for some patients with severe spasticity (4, 5).
Chemoneurolysis via localized injections can help provide focal spasticity relief (1, 3, 6). In addition, the use of single-event multi-level chemoneurolysis helps treat several areas of muscle spasticity, each with varying severities (7). Medications used in chemo-neurolysis procedures include botulinum neurotoxin (BoNT), phenol, and alcohol neurolysis (3–7). Compared with phenol and the understudied alcohol neurolysis, BoNT usage in treating spasticity is documented extensively in the literature with regards to pharmacodynamics, adverse effects and clinical benefits (7–9). However, the response to chemodenervation with BoNT often requires 3–5 days to generate spasticity benefit, which generally lasts approximately 3 months. Although clinical standards permit repeating chemodenervation every 3 months, the majority of patients with spasticity prefer an increased frequency for maintaining clinical benefit (10–12). BoNT injections are associated with significant costs, and repeated injections are often further restricted by financial feasibility. In the USA, depending on the insurance being used, the approved dosage of BoNT is only 400–600 units of every 3 months. These limitations prevent the sole utility of chemodenervation for a multi-pattern treatment, e.g. elbow flexion, clenched fist, stiff knee gait, and equinovarus of the foot. Consequently, phenol neurolysis (PN) and BoNT are used in complement, with PN frequently reserved for proximal nerves and BoNT used for distal musculature.
In contrast, PN produces an almost-immediate effect that manifests within minutes of injection, which may last as long as 6 months depending on the dosage used (1, 13). In addition, PN is significantly less expensive. PN may also be re-injected before 3 months, unlike BoNT. However, the safety and efficacy of PN is less-commonly documented in the literature than BoNT chemodenervation. PN also requires a higher level of expertise to administer, and has a worse side-effect profile, which includes hypotension, prolonged pain, dysaesthesias, site inflammation, and joint fibrosis (1, 13, 14). These disadvantages for phenol usage are associated with safety concerns relative to neurotoxins, thus making BoNT a vastly more popular option for chemoneurolysis. Phenol is therefore being used increasingly less in the USA and is poorly documented in the spasticity literature. Given its advantages, PN may be superior to chemodenervation with BoNT in certain clinical scenarios. Thus, the primary purpose of the current study is to describe the utilization pattern of PN at a single site.
Posted by Kostas Pantremenos in Uncategorized on June 27, 2017

By Stephanie Miller, PT
I’ll admit it: I’m excited about all that I can do with PTNow. This is somewhat unusual for me, because I’ve always felt a little daunted by technology (see my first post for more on that).
But this thing is awesome.
And yet, the fact that PTNow is so awesome—that it contains so much information—can feel a little … overwhelming. I mean, where do you start? How do you start?
Here’s how I got my feet wet, and a few tips based on what I’ve learned along the way.
To begin with, I decided early on that I’d focus on small chunks, and get comfortable with bits and pieces at a time. I mean, anything new I learn today is more than I knew yesterday, right? Since I’d like to do a better job at searching articles, I thought ArticleSearch would be a good place to start. Seemed easy enough.
As heart failure is a common diagnosis in my practice area of home health, I decided to search on that topic. I began with the “basic search” option. The search window is what you’d expect: a box in which you can type in whatever search terms you’re looking for.
But then came the challenging part … all of the databases. ArticleSearch lets you choose which databases you want to use in your search, and although I vaguely recognized a few from grad school, I hated to admit that a lot of them were foreign to me. But where there’s a will, there’s a way! I was determined to understand the value of each and identify why I would select one over the other. Fortunately, the PTNow tutorial video helps to explain the differences.
The abstracts to the best articles are found using the Cumulative Index to Nursing and Allied Health Literature (CINAHL), ProQuest Health and Medical Complete, ProQuest Nursing and Allied Health Source, and SPORTDiscus. There are differences between them. Here’s a quick comparison, based on what I learned from the PTNow tutorial.
CINAHL
ProQuest Nursing and Allied Health Source
ProQuest Health and Medical Complete
SPORTDiscus
Cochrane Database of Systematic Reviews
If you’re looking for a specific kind of research resource, here’s what the tutorial suggests:
Full-text articles
CINAHL Complete, Proquest Nursing and Allied Health Source, Proquest Health and Medical Complete, SPORTDiscus (be sure to select the “full-text only” option on the search page)
Systematic reviews
Cochrane Database of Systematic Reviews
Physical therapy-specific research
CINAHL Complete, Proquest Nursing and Allied Health Source, Proquest Health and Medical Complete
Sport-related information
SPORTDiscus
As for my own search …
After becoming more comfortable with the benefits of each database, I decided that the Cochrane database was the place I wanted to begin my investigation into the effects of exercise on patients with congestive heart failure. I clicked on the link, typed in “effects of exercise on patients with congestive heart failure” in the search bar, and chose the Cochrane database. In a few seconds I found articles on the beneficial effects of combined exercise training on early recovery, the effects of specific inspiratory muscle training on the sensation of dyspnea and exercise tolerance, the role resistance exercise training can play in improving heart function and physical fitness in stable patients with heart failure, and the effects of short-term exercise training and activity restriction on functional capacity in patients with severe chronic congestive heart failure, to name just a few. Wow.
Through this whole experience, I not only learned some of the details of how ArticleSearch works, I also got a better sense of how to get the most out of my searches. I suggest a few general tips:
If, like me, you sometimes wrestle with technology, you’ll understand this mixed bag I feel when I’m faced with something outside my technological comfort zone: I know technology can make my professional life easier, but I worry that the technology itself won’t be easy. I was happily mistaken with ArticleSearch. It was so easy!
How easy? Let me put it this way—I have a lot of reading to do.
Stephanie Miller is a staff development specialist with Celtic Healthcare.
Source: Confessions of a Tech-Challenged PT: Asking Searching Questions – And Getting Useful Answers
Posted by Kostas Pantremenos in Paretic Hand on June 27, 2017
Prospective, repeated-measures study.
Understanding individual hand function can assist therapists with the process of determining relevant treatment approaches and realistic therapeutic outcomes. At this point in time, a composite test that assesses both unilateral and bimanual hand function in relation to a functional activity is not available.
To establish the reliability and validity of the suitcase packing activity (SPA).
An expert panel established face and content validity. Eighty healthy, English-speaking volunteers aged between 18 and 45 years were randomly assigned to either 1 or 2 sessions (test-retest reliability). Relative agreement between 2 examiners using an intraclass correlation coefficient (ICC)3,1 determined interrater reliability. Test-retest reliability was determined by using a repeated-measures analysis of variance and an ICC3,2. Concurrent validity was evaluated against 2 well-established hand evaluations using separate tests of correlational coefficients.
Face and content validity were established across 4 focus groups. Our results demonstrate good to excellent interrater reliability (ICC3,1 ≥ 0.93) and good to excellent test-retest reliability (ICC3,2 ≥ 0.83). SPA scores were moderately correlated with the 2-hand evaluations.
Through evaluating hand function during participation in a goal-directed activity (eg, packing a suitcase), the SPA exhibits promise in usefulness as a future viable outcome measure that can be used to assess functional abilities following a hand injury.
The SPA is a valid and reliable tool for assessing bimanual and unilateral hand function in healthy subjects.
Source: The suitcase packing activity: A new evaluation of hand function – Journal of Hand Therapy
Posted by Kostas Pantremenos in Functional Electrical Stimulation (FES), Gait Rehabilitation - Foot Drop on June 27, 2017
Foot drop can be defined as an abnormality in the gait where the forefoot drops due to factors such as weakness of the ankle and toe dorsiflexion. The abnormality is also caused by paralysis of the muscles in the anterior portion of the lower leg or damage to the fibular nerve. Foot drop can be associated with various conditions, including peripheral nerve injuries, neuropathies, drug toxicities, dorsiflexor injuries, and diabetes. Anatomic, muscular, and neurologic are the three categories of foot drop.
Functional electrical stimulation technology is employed in the foot drop implant to improve the gait of patients and avoid foot drop or tripping while walking. Functional electric stimulators (FES) can either be implanted within the patient’s body or employed externally. External FES is tested on the patient prior to its implantation. Implant FES involves a surgery in which the electrodes are directly placed on the nerves of the patient, which are controlled by the implant placed under the skin. The FES device activates the implant through a wireless antenna that is worn outside the body. Sensors are also associated with FES which trigger events in the walking pattern such as lifting of the heel, thereby stimulating the nerves.
The advantages of implant FES include reduction in sensation that is associated with external stimulation. In addition, it eliminates the need to adjust the electrodes on the skin on a daily basis. Rise in number of foot drop disorders due to nerve injuries, growth in knee and hip replacement therapies that lead to foot drop disorders, and increase in the number of sports related injuries contribute to the growth of the foot drop implants market. Foot drop disorders are commonly observed in diabetic retinopathy patients and this prevalence is growing due to increase in incidence of diabetes, which is propelling the growth of the market. Furthermore, the market players are focus on research and development to increase the number of foot drop implant products available in the market, driving the market growth. However, lack of reimbursement, high cost of the implants, and low awareness among the people are likely to hinder the growth of the foot drop implants market in the near future.
Get Sample Copy of this Report @ http://www.transparencymarketresearch.com/sample/sample.php?flag=B&rep_id=22913
The global foot drop implants market can be segmented on the basis of product, end-user, and region. On the basis of product, the market is categorized into functional electrical stimulators and internal fixation devices. The internal fixation devices segment is anticipated to record a significant growth during the forecast period owing to increasing demand for the devices and advantages offered by these devices such as elimination of the need to stimulate the electrodes daily. Based on end-user, the market can be segmented into hospitals, orthopedic centers, and palliative care centers, among others. The orthopedic centers segment is anticipated to record a high growth during the forecast period due to the increasing number of foot drop cases due to injuries.
Geographically, the foot drop implants market is distributed over North America, Latin America, Europe, Asia Pacific, and Middle East & Africa. North America dominated the market in 2016 and is anticipated to continue its dominance during the forecast period. The significant growth of the market in the region can be attributed to the strong focus on research and development, increase in health care spending, and growth in awareness about the abnormality. The sluggish economy might have a negative impact on the market growth of Europe. Asia Pacific is anticipated to record a high CAGR during the forecast period, primarily driven by India and China. The rising disposable income is anticipated to contribute to the growth of the Asia Pacific market. In addition, a factor contributing to the market growth is rise in prevalence of diabetes that leads to diabetic retinopathy, which is one of the primary causes of foot drop.
View Report @ http://www.transparencymarketresearch.com/foot-drop-implants-market.html
Key players operating in the foot drop implants market include Finetech Medical, Arthrex, Inc., Zimmer Biomet, Bioness Inc., Stryker Corporation, Wright Medical Group N.V., Ottobock, Narang Medical Limited, PONTiS Orthopaedics, LLC, and Shanghai MicroPort Orthopedics.
About Us
Transparency Market Research (TMR) is a market intelligence company, providing global business information reports and services. Our exclusive blend of quantitative forecasting and trends analysis provides forward-looking insight for thousands of decision makers. TMR’s experienced team of analysts, researchers, and consultants, use proprietary data sources and various tools and techniques to gather, and analyze information. Our business offerings represent the latest and the most reliable information indispensable for businesses to sustain a competitive edge.
Each TMR syndicated research report covers a different sector – such as pharmaceuticals, chemicals, energy, food & beverages, semiconductors, med-devices, consumer goods and technology. These reports provide in-depth analysis and deep segmentation to possible micro levels. With wider scope and stratified research methodology, TMR’s syndicated reports strive to provide clients to serve their overall research requirement.
US Office Contact
90 State Street, Suite 700
Albany, NY 12207
Tel: +1-518-618-1030
USA – Canada Toll Free: 866-552-3453
Source: Foot Drop Implants Market Analysis and Forecasts 2025 | Medgadget
Posted by Kostas Pantremenos in Gait Rehabilitation - Foot Drop on June 27, 2017
Source: Advanced Gait Analysis: Insights into Human Locomotor Control (PDF Download Available)
Posted by Kostas Pantremenos in Paretic Hand, Tele/Home Rehabilitation on June 27, 2017
A total of 80% of stroke cases result in hemiparesis,1 and half this number experience persistent lack of arm function.2 Effective interventions are lacking, and evidence to support those that are accessible is insufficient.3 A clear need has been identified for long-term support in the community for people with stroke, but services are limited and few studies have examined home-based interventions and provided sufficient detail of the protocols used.4
Music interventions may be beneficial for improving arm function following stroke,5,6 and a strong rhythmic stimulus embedded within music may enhance motor performance more than the use of a rhythmic stimulus alone without music.7 More research is needed to establish the effects of music interventions on arm function, and with the majority of rehabilitation being delivered in patients’ homes it is useful to determine the feasibility of home-based treatment delivery and research. This article reports on the feasibility of conducting a randomized controlled trial where a music intervention, for which there was a clear protocol based on published guidelines,8,9 was delivered in a variety of home environments.[…]
Figure 1. Study flow diagram. Data collection occurred at weeks 1, 6, 9, 15 and 18. Cross-over analysis required data from weeks 1, 6, 9 and 15.
Posted by Kostas Pantremenos in Disability and Sex, Educational, TBI on June 27, 2017
By Xavier Figueroa, Ph.D.
http://www.msktc.org/tbi/factsheets/Sexuality-After-Traumatic-Brain-Injury
 What is the largest sex organ in the body?
What is the largest sex organ in the body?
The brain, of course! (Followed by the spinal cord ganglia but let’s not judge).
Intimacy, desire, physical contact and pleasure, they are very basic needs in a relationship. Marriages, partnerships and friendships rely on this most basic link. But when a brain injury occurs, changes in desire and drive (hypo- and hyper-sexuality) can become apparent. Energy and mood can also be affected, which can induce a change in libido, interest and desire. Damage to certain portions of the brain may affect your ability to move, reducing spontaneity and self-esteem. Elements of coming to terms with the trauma, such as shock and recovery may take time, as well as recovery from physical rehabilitation. If the injury is chronic, other changes may become apparent, including cognitive and behavioral changes that shift how friends and partner interact with each other.
Much of these changes can occur days, weeks or even months after the injury, even in mild to moderate traumatic brain injuries. Knowing how to identify, adapt and overcome the changes associated with an ABI/TBI is an important part of recovery.
The most important information to take away from this post is the following: you are not alone, you are not abnormal and you will get better. Millions of individuals and couples have gone through the recovery of a brain injury and difficulties with reestablishing a functional sexual relationship. Hang in there.
When we talk about sex, we are talking about something that is simple in practice, but complex in execution. Prior to the brain injury, a pattern of behavior between yourself and your partner was established. How you interacted and what you expected prior to and leading to sexual intimacy were established and anticipated. I wouldn’t call it a pattern (that’s not very exciting!), but a role in which you knew which part each one would play.
A brain injury directly affects the biggest and most important sex organ in the human body. It’s no wonder that sexual issues appear in 50-60% of people that suffer a moderate to severe TBI. In a recent article in US News and World Report (Health Day, April 29, 2013; Link) that reported on the study that appeared in NeuroRehabilitation: An International Journal:
‘The study found that 50 percent to 60 percent of people with TBI have sexual difficulties, such as reduced interest in sex, erectile dysfunction, pain during sex, difficulties in vaginal lubrication, difficulties achieving orgasm or staying aroused, and a sense of diminished sex appeal, Moreno said.
The research found that partners of those with TBI experienced personality and emotional changes, and a modification of family roles that can lead to a crisis, Moreno said. “For the spouse, the survivor becomes a different person, a person they do not recognize as the one they fell in love with in the past,” he said. “The spouse becomes a caregiver and this imbalance in the relationship directly affects sexual desire.”’
Even in cases of mild TBI, there are incidences of 25-50% of people experiencing sexual difficulties [1], especially in individuals exposed to bomb-blast injuries. Brain injuries are not mild…they can take a life of their own and totally transform who you are and how you relate to your significant other (spouse, partner or lover). Many of these changes can be divided into 5 major groups:
But these are just the changes that occur with sexual interaction (as if that weren’t enough). These are behavioral changes that hide deeper and more profound changes that can occur throughout the body. Changes in sexual desire are like the proverbial canary in the coal mine…it warns you that something is amiss.
Damage to the brain can induce a number of changes:
Fatigue/Tiredness
Hormonal Changes
Emotional Changes
Cognitive Changes
Spasticity/Movement Problems
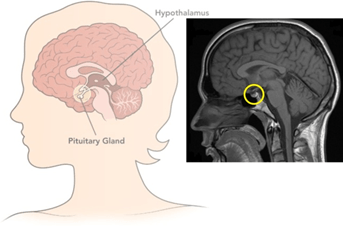
These changes can come from very specific damage to certain areas of the brain, such as your pituitary, the frontal and temporal lobes of the brain. When you get down to it, sex is a very complicated process…neurologically speaking! A number of body systems have to work together to make the engines of desire go vroom…and when one system is not working, then it can cause the engine to misfire and stall.
The pituitary gland is a tiny portion of the brain… but don’t let its size fool you. It is a master regulator of hormones that, when damaged, can diminish your ability to regulate your blood pressure, sleep cycle and hormones.
 The function of the pituitary is diverse, as it can affect a number of really important functions:
The function of the pituitary is diverse, as it can affect a number of really important functions:
Hormones secreted from the pituitary gland help control the following body processes:
If that weren’t enough, this can cascade into disease states that may not seem related to a TBI. One thing that we are seeing with returning veterans is pituitary dysfunction is present and undiagnosed or under diagnosed. Even with hormone or growth factor replacement therapies, a pituitary that is not firing on all cylinders will continue to cause long-term problems. Although changes in sexual interaction are the most visible and can be due to pituitary damage, they warn that the damage is more profound. The Big Organ (the brain) has a lot of functions related to behavior…and when it comes to sex, behavior is key (good or bad).
This portion of the brain, the hypothalamus, is a close neighbor to the pituitary. So close, they are friends with benefits. One of the most important functions of the hypothalamus is to link the nervous system to the endocrine system via the pituitary gland (another name of the pituitary is the hypophysis).
The hypothalamus is more of a region than an actual structure. It is composed of many groups of neurons (called nuclei) that control a wide variety of hormonal secretions and behaviors. In a recent small scale study of severe TBI, it was discovered that ~21% of study subjects suffered from hypothalamic-hypophysial dysfunction. In about 40% of male TBI sufferers, there was a detectable drop in testosterone levels [2], which can affect sexual drive and desire in men. About 15% of all patients with a TBI have some degree of hypopituitarism that can go unrecognized and could be mistakenly ascribed to persistent neurologic injury and cognitive impairment [3].
The reason for the hypothalamic damage being mistaken for neurologic injury and cognitive impairment are due to the very broad effects that the hypothalamus exerts on metabolism and brain function. If the hypothalamus is misfiring, it takes a very involved physician (or physicians), with training in neurology, endocrinology and/or experience with TBI to identify the problem. A lot of systems can malfunction in a brain injury.

The frontal lobe (in green) • tumblr
In head injuries, damage to the frontal lobe is thought to occur frequently. Car crashes (especially front end collisions, are thought to cause frontal and occipital lobe damage. Damage to the frontal lobe has been reported to cause individuals to behave inappropriately in response to normal social situations. Loud or overly-boisterous exchanges, inappropriate genital touching (in public) or fixation on one subject or person have been reported outcomes after a TBI. Changes in emotional affect (expression of emotions) that are felt may not be expressed in the face or voice. For example, someone who is feeling happy would not smile, and his or her voice would be devoid of emotion. This can be very disconcerting to a partner and can be experienced a loss of affection or interest. How a partner or loved one that is a caretaker of a TBI victim experiences the injury will have a direct effect on their own sexual desire and interest.
Along the same lines, though, the person may also exhibit excessive, unwarranted displays of emotion or poor control of anger. Poor anger management is associated with some forms of frontal lobe damage. Depression is not an uncommon outcome from a head injury, especially if there is frontal lobe damage. Also common along with depression is a loss of or decrease in motivation. Someone might not want to carry out normal daily activities and would not feel “up to it”. Sex might not seem as interesting or motivating.
Those who are close to the person who has experienced the damage may notice that the person no longer behaves like him or herself. The frontal lobe is the same part of the brain that is responsible for executive functions such as planning for the future, judgment, decision-making skills, attention span, and inhibition. These functions can decrease drastically in someone whose frontal lobe is damaged. A short list of behavioral changes associated with frontal lobe damage is given below:
Frontal lobe damage is only one part of cerebral cortex, but is the most common type of cortical damage due to a TBI. Other parts may be damaged as well. Frontal lobe damage is common and better associated with impulse and emotional control, making sufferers act completely out of character and unable to control or edit themselves or their responses.
So, after reading all of this, what does it do for you? How does this help you re-establish the emotional, sexual and intimate relationship you wish with your partner? As a caretaker, or as a sufferer, the TBI is a big elephant in the room. It exists; it takes up space in your life, even though it can’t be seen. The person you knew is not present…they have not come back from their injury and they might not come back. Some do recover, others do not. But you can still create a new bond, a new relationship and a new life. And you can fight to repair the damage to the brain.
There are limited options for therapy in current medical practice. Mostly, it is focused on developing new skills, relearning old ones, developing coping skills or taking medications. That’s just for the TBI sufferer, not the caretaker(s). The complexity and variety of problems that pop-up when dealing with a brain injury are truly staggering and expensive. Fortunately, the majority of mild-to-moderate TBI’s do recover. Patience and persistence in therapy are required in order to make a recovery.
Unfortunately, for a portion of all TBI sufferers, recovery may take years. That is a long-time to wait. Therapies that help to re-build the brain connections (neuroplasticity) or restore blood flow to the brain hold promise for restoring function again. Hyperbaric oxygen therapy (HBOT) is one such therapy that has a good number of clinical studies to support its use for chronic TBI and PCS [4-9]. Near infra-red and infra-red technologies show promise for a TBI therapy, as well [10-13].
Nutritional support, such as Omega-3 fatty acids (DHA and EPA), has shown the ability to reduce the long-term neuroinflammation associated with a TBI [14-16] and help with white matter repair. Other nutritional therapies may exist to help mediate repair in a TBI.
The take home message is that there are potential therapies that are being developed to help treat the neurological damage of a TBI. Take heart that the “new normal” for yourself or your loved one may not need to be permanent.
Disclaimer: I am not a medical doctor. I am not giving medical advice, diagnosis or treatment recommendations. The posts on this blog are my opinion. If you are thinking of following or using any of this information for any health related conditions, I would recommend you talk to your physician and seek guidance and help. I try to be as meticulous as possible in the information I use for these posts. I look for potential therapies that are low-risk/high impact. There are no guarantees, but knowledge is power and self-direction can lead you to uncover and do incredible things.
Source: Brain Injury and Sex: What Happens After a TBI? | Brain Health & Healing Foundation
You are currently browsing the archives for June, 2017

