Posts Tagged Transcranial magnetic stimulation
[ARTICLE] Upper Limb Function Recovery by Combined Repetitive Transcranial Magnetic Stimulation and Occupational Therapy in Patients with Chronic Stroke According to Paralysis Severity – Full Text
Posted by Kostas Pantremenos in Paretic Hand, tDCS/rTMS on February 12, 2023
Abstract
Repetitive transcranial magnetic stimulation (rTMS) with intensive occupational therapy improves upper limb motor paralysis and activities of daily living after stroke; however, the degree of improvement according to paralysis severity remains unverified. Target activities of daily living using upper limb functions can be established by predicting the amount of change after treatment for each paralysis severity level to further aid practice planning. We estimated post-treatment score changes for each severity level of motor paralysis (no, poor, limited, notable, and full), stratified according to Action Research Arm Test (ARAT) scores before combined rTMS and intensive occupational therapy. Motor paralysis severity was the fixed factor for the analysis of covariance; the delta (post-pre) of the scores was the dependent variable. Ordinal logistic regression analysis was used to compare changes in ARAT subscores according to paralysis severity before treatment. We implemented a longitudinal, prospective, interventional, uncontrolled, and multicenter cohort design and analyzed a dataset of 907 patients with stroke hemiplegia. The largest treatment-related changes were observed in the Limited recovery group for upper limb motor paralysis and the Full recovery group for quality-of-life activities using the paralyzed upper limb. These results will help predict treatment effects and determine exercises and goal movements for occupational therapy after rTMS.
1. Introduction
Motor paralysis after stroke limits patients’ activities of daily living (ADL) and reduces their quality of life [1,2]. Recently, noninvasive brain stimulation therapy has been developed to improve patients’ motor paralysis and ADL, and its effectiveness has been demonstrated [3,4]. The treatment of upper limb motor paralysis involves modulation of interhemispheric inhibition and induction of neuroplasticity in the cerebrum. A novel intervention using repetitive transcranial magnetic stimulation (rTMS) in combination with intensive occupational therapy (NEURO) has recently been developed [5]. In patients with stroke hemiplegia, high-frequency rTMS has been applied to the hemisphere ipsilateral to the paralysis to increase excitability [6], and low-frequency rTMS has been applied to the contralateral hemisphere to decrease interhemispheric inhibitory connections [7,8] with the damaged cortex [9]; thus, both high-frequency rTMS and low-frequency rTMS have been applied [10]. Repetitive currents are induced in the brain cortex to produce long-term changes in cortical excitability. In acute patients, high-frequency (10 Hz) rTMS applied to the impaired motor cortex activates it, improving paralysis [11,12]. In occupational therapy after rTMS, the patients in whom the activation of the interhemispheric inhibitory motor cortex has been adjusted are prescribed repetitive joint movements. The aim is to promote use-dependent plasticity in the brain and to subsequently restore motor paralysis and improve ADL [13]. NEURO is an effective treatment for improving upper limb dysfunction and impairments in ADL in chronic stroke patients 6 months after stroke onset. Its therapeutic effect has been shown to be unaffected by stroke type (cerebral hemorrhage or cerebral infarction) [14].
The goal of NEURO is to improve the quality of movement of the patient’s paralyzed upper limb by allowing it to be used in ADL. Since the effectiveness of NEURO depends on the severity of motor paralysis, therapists determine the exercises and target movements based on the patient’s pre-treatment upper limb function assessment score. The Fugl–Meyer Assessment of the Upper Extremity (FMAUE) and the Action Research Arm Test (ARAT) are used to assess upper limb motor function outcomes in NEURO [15]. These evaluation methods have been shown to have high accuracy and clinical usefulness. A previous study has been conducted to estimate post-treatment scores from the pre-NEURO FMAUE score [16]. The ARAT is a functional upper limb assessment tool used in patients with post-stroke hemiplegia and is characterized by its ability to reflect the patient’s activity [17]. Since the ARAT consists of object manipulation and reaching tasks, the occupational therapist (OT) plans exercises by estimating the ADLs in which the patient can use their hands based on the obtained assessment results. As the ARAT score correlates with the Motor Activity Log, which investigates the use of the paralyzed limb in ADLs, OTs helping patients improve their activity limitations can use it as a reference value for exercises and goal-setting [18,19]. Therefore, it can be inferred that predicting treatment effects with ARAT is more advantageous than using FMAUE in setting treatment goals and planning effective ADL exercises for patients. If ARAT scores are found to improve with NEURO, it will be easier for OTs to pre-determine the content of ADL exercises and develop achievable ADL goals.
Patients with mild-to-moderate motor paralysis with FMAUE scores ≥43 have higher interhemispheric inhibition from the healthy hemisphere to the affected hemisphere. It is predicted that the therapeutic effect of upper limb practice in the presence of rTMS-induced changes in synaptic transmission efficiency is dependent on motor paralysis severity [20]. If the post-treatment effects according to motor paralysis severity can be predicted using pre-treatment ARAT scores, the target movements for patients could be set with high accuracy. Recently, a treatment method using a brain-computer interface (BCI) was developed for the rehabilitation of stroke patients, and its effectiveness has been reported [21,22]. Even for new intervention methods, it is better to formulate exercises adapted to the severity of paralysis and recovery. Therefore, the results obtained in this study can be used as data to plan the most appropriate practice for patients in terms of future new intervention methods. As a result, this study aimed to estimate the amount of change in ARAT scores for each level of motor paralysis severity, classified according to the ARAT score before NEURO. […]
[ARTICLE] Short-term Effect of Noninvasive Brain Stimulation Techniques on Motor Impairment in Chronic Ischemic Stroke: A Systematic Review with Meta-Analysis – Full Text
Posted by Kostas Pantremenos in Paretic Hand, tDCS/rTMS on March 8, 2022
Abstract
Background: In recent years, noninvasive brain stimulation (NIBS) has shown promise for stroke rehabilitation as a novel nonpharmaceutical neuromodulatory intervention with attractive neurophysiological theories backing it up.
Objective: To find out the short-term effects of NIBS techniques on motor impairment in chronic ischemic stroke.
Materials and Methods: A systematic review with meta-analysis was performed separately for transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), and studies that combined both, utilizing various databases for a period spanning from 2001 to 2019. Good-quality randomized controlled trials (RCTs) on chronic ischemic stroke cases with homogeneous clinical upper motor short-term outcome measures were considered for the meta-analysis. RevMan 5.1 software was used for the meta-analysis. Meta-analysis registration: CRD42021196299; https://www.crd.york.ac.uk/PROSPERO
Results: A total of 319 studies were identified initially. After necessary filters to comply with the strict recruitment criteria, only four studies qualified, two each for tDCS and TMS and none qualified for analysis under the combined category. tDCS showed a nonsignificant effect on the upper limb motor function improvement (−0.10 [95% confidence interval {CI}: −0.84 to 0.64; I2 0%; P = 0.8]), whereas the repetitive TMS showed a significant effect (0.75 [95% CI: 0.03–1.48; I2 0%; P = 0.04]). The safety analysis did not reveal any major concerns for several published protocols.
Conclusions: tDCS alone did not significantly benefit motor recovery; rTMS was effective in providing immediate functional benefits in chronic ischemic stroke. While the current stroke rehabilitation protocols with NIBS appear safe, more good-quality stratified RCTs with more innovative experimental protocols are needed to analyze and quantify the efficacy of these techniques in stroke rehabilitation.
—————————
Stroke is a sudden nonconvulsive focal neurological deficit of vascular etiology due to infarction or hemorrhage into brain or spinal cord parenchyma in the anterior or posterior circulation territories. Around 15 million people worldwide suffer from stroke every year. Stroke is the leading cause of adult disability in the elderly, and it leaves around a third of victims permanently disabled. Contingent upon the site and the extent of the brain lesion, post-stroke disabilities vary in survivors, and rehabilitation measures are important to improve the quality of life in stroke survivors. Early rehabilitation is the key for recovery and involves multidisciplinary approaches. However, conventional stroke rehabilitation seldom succeeds in achieving a good recuperation in a vast majority of the cases. Only few rehabilitation techniques have gold standard protocols, and this holds especially true for several newly evolving technologies. Neuromodulation methods such as noninvasive brain stimulation (NIBS) include transcranial electrical stimulation (TES) which in turn can be direct or alternate current stimulation (tDCS/ACS) and transcranial magnetic stimulation (TMS) which all have now been intensively investigated as facilitatory or inhibitory types of stimulations[1] to induce desirable priming effects for routine neurorehabilitation.
A Cochrane review published in 2013 reported unimpressive effects on motor improvement with repetitive transcranial magnetic stimulation rTMS and partly attributed it to the heterogeneity of the trials.[2] This study covered publications only till 2012, but analysed 19 trials involving a total of 588 participants. It reported meta-analysis of two heterogenous trials with a total of 183 participants which showed rTMS treatment not being associated with any significant increase in the functional status after stroke with a Barthel index score mean difference (MD) of 15.92 with 95% confidence interval (CI) of − 2.11 to 33.95. Four other trials with a total of 73 participants also did not find any statistically significant effect on motor function with MD of 0.51 and 95% CI of − 0.99 to 2.01. Subgroup analyses of different stimulation frequencies or duration of illness also showed no significant difference. But they reported that the adverse events (AEs) in the rTMS groups were mild, with the most common event being transient or mild headaches (2.4%) and local discomfort at the site of the stimulation. They concluded against the routine use of rTMS for the treatment of stroke and recommended further trials with larger sample sizes to determine a suitable rTMS protocol and the long-term functional outcome. Another meta-analysis reported in 2016 covered 23 studies till 2015 and generated 29 comparisons: 14 on tDCS and 15 on rTMS. Using random-effects models, they indicated improvements in paretic limb force after tDCS and rTMS rehabilitation. They reported positive effects on force production with two stimulation protocols, one on increasing cortical activity in the ipsilesional hemisphere and the other on decreasing cortical activity in the contralesional hemisphere. They also reported improved reduction of force across acute, subacute, and chronic phases of stroke with both tDCS and rTMS. While the first meta-analysis was a Cochrane review, the second was a publication in a more technical journal, Brain Stimulation. But the differences between the conclusions are obviously most striking. It is, therefore, important to revisit the studies till date, including those conducted from 2016 till date, and make sense of the reports of quality studies through a fresh systematic review. In order to avoid too much of heterogeneity which makes meta-analysis difficult, we confined our studies to randomized controlled trials (RCTs) of NIBS on upper limb motor rehabilitation in chronic ischemic stroke patients and aimed to determine the effectiveness and safety through a systematic review.[…]
[WEB] Neuroimaging technology used to study how brain stimulation works for treatment of depression
Posted by Kostas Pantremenos in Depression, Radiology/Imaging technology on May 13, 2021
Reviewed by Emily Henderson, B.Sc. May 4 2021
Repetitive transcranial magnetic stimulation, or rTMS, was FDA approved in 2008 as a safe and effective noninvasive treatment for severe depression resistant to antidepressant medications. A small coil positioned near the scalp generates repetitive, pulsed magnetic waves that pass through the skull and stimulate brain cells to relieve symptoms of depression. The procedure has few side effects and is typically prescribed as an alternative or supplemental therapy when multiple antidepressant medications and/or psychotherapy do not work.
Despite increased use of rTMS in psychiatry, the rates at which patients respond to therapy and experience remission of often-disabling symptoms have been modest at best.
Now, for the first time, a team of University of South Florida psychiatrists and biomedical engineers applied an emerging functional neuroimaging technology, known as diffuse optical tomography (DOT), to better understand how rTMS works so they can begin to improve the technique’s effectiveness in treating depression. DOT uses near-infrared light waves and sophisticated algorithms (computer instructions) to produce three-dimensional images of soft tissue, including brain tissue.
Comparing depressed and healthy individuals, the USF researchers demonstrated that this newer optical imaging technique can safely and reliably measure changes in brain activity induced during rTMS in a targeted region of the brain implicated in mood regulation. Their findings were published April 1 in the Nature journal Scientific Reports.
This study is a good example of how collaboration between disciplines can advance our overall understanding of how a treatment like TMS works. We want to use what we learned from the application of the diffuse optical tomography device to optimize TMS, so that the treatments become more personalized and lead to more remission of depression.”
Shixie Jiang, MD, study lead author, third-year psychiatry resident, USF Health Morsani College of Medicine
DOT has been used clinically for imaging epilepsy, breast cancer, and osteoarthritis and to visualize activation of cortical brain regions, but the USF team is the first to introduce the technology to psychiatry to study brain stimulation with TMS.
“Diffuse optical tomography is really the only modality that can image brain function at the same time that TMS is administered,” said study principal investigator Huabei Jiang, PhD, a professor in the Department of Medical Engineering and father of Shixie Jiang. The DOT imaging system used for USF’s collaborative study was custom built in his laboratory at the USF College of Engineering.
The researchers point to three main reasons why TMS likely has not lived up to its full potential in treating major depression: nonoptimized brain stimulation targeting; unclear treatment parameters (i.e., rTMS dose, magnetic pulse patterns and frequencies, rest periods between stimulation intervals), and incomplete knowledge of how nerve cells in the brain respond physiologically to the procedure.
Related Stories
- Cardiovascular risk factors accumulated from childhood linked to poorer brain function at midlife
- Covid-19 patients show reduced gray matter volume in the brain
- New imaging technique captures real-time brain motion in stunning detail
Portable, less expensive, and less confining than some other neuroimaging equipment like MRIs, DOT still renders relatively high-resolution, localized 3D images. More importantly, Dr. Huabei Jiang said, DOT can be used during TMS without interfering with treatment’s magnetic pulses and without compromising the images and other data generated.
DOT relies on the fact that higher levels of oxygenated blood correlate with more brain activity and increased cerebral blood flow, and lower levels indicate less activity and blood flow. Certain neuroimaging studies have also revealed that depressed people display abnormally low brain activity in the prefrontal cortex, a brain region associated with emotional responses and mood regulation.
By measuring changes in near-infrared light, DOT detects changes in brain activity and, secondarily, changes in blood volume (flow) that might be triggering activation in the prefrontal cortex. In particular, the device can monitor altered levels of oxygenated, deoxygenated, and total hemoglobin, a protein in red blood cells carrying oxygen to tissues.
The USF study analyzed data collected from 13 adults (7 depressed and 6 healthy controls) who underwent DOT imaging simultaneously with rTMS at the USF Health outpatient psychiatry clinic. Applying the standard rTMS protocol, the treatment was aimed at the brain’s left dorsolateral prefrontal cortex – the region most targeted for depression.
The researchers found that the depressed patients had significantly less brain activation in response to rTMS than the healthy study participants. Furthermore, peak brain activation took longer to reach in the depressed group, compared to the healthy control group.
This delayed, less robust activation suggests that rTMS as currently administered under FDA guidelines may not be adequate for some patients with severe depression, Dr. Shixie Jiang said. The dose and timing of treatment may need to be adjusted for patients who exhibit weakened responses to brain stimulation at baseline (initial treatment), he added.
Larger clinical trials are needed to validate the USF preliminary study results, as well as to develop ideal treatment parameters and identify other dysfunctional regions in the depression-affected brain that may benefit from targeted stimulation.
“More work is needed,” Dr. Shixie Jiang said, “but advances in neuroimaging with new approaches like diffuse optical tomography hold great promise for helping us improve rTMS and depression outcomes.”
[ARTICLE] Evidence of neuroplasticity with robotic hand exoskeleton for post-stroke rehabilitation: a randomized controlled trial – Full Text
Posted by Kostas Pantremenos in Neuroplasticity, Paretic Hand, REHABILITATION, Rehabilitation robotics on May 9, 2021
Abstract
Background
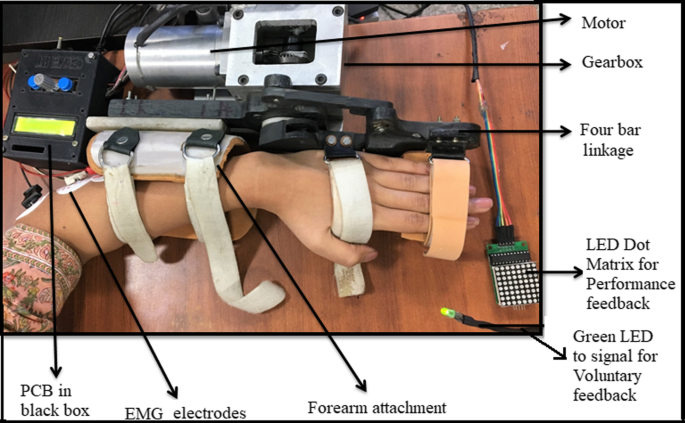
A novel electromechanical robotic-exoskeleton was designed in-house for the rehabilitation of wrist joint and Metacarpophalangeal (MCP) joint.
Objective
The objective was to compare the rehabilitation effectiveness (clinical-scales and neurophysiological-measures) of robotic-therapy training sessions with dose-matched conventional therapy in patients with stroke.
Methods
A pilot prospective parallel randomized controlled study at clinical settings was designed for patients with stroke within 2 years of chronicity. Patients were randomly assigned to receive an intervention of 20 sessions of 45 min each, five days a week for four weeks, in Robotic-therapy Group (RG) (n = 12) and conventional upper-limb rehabilitation in Control-Group (CG) (n = 11). We intended to evaluate the effects of a novel exoskeleton based therapy on the functional rehabilitation outcomes of upper-limb and cortical-excitability in patients with stroke as compared to the conventional-rehabilitation. Clinical-scales– Modified Ashworth Scale, Active Range of Motion, Barthel-Index, Brunnstrom-stage and Fugl-Meyer (FM) scale and neurophysiological measures of cortical-excitability (using Transcranial Magnetic Stimulation) –Motor Evoked Potential and Resting Motor threshold, were acquired pre- and post-therapy.
Results
No side effects were noticed in any of the patients. Both RG and CG showed significant (p < 0.05) improvement in all clinical motor-outcomes except Modified Ashworth Scale in CG. RG showed significantly (p < 0.05) higher improvement over CG in Modified Ashworth Scale, Active Range of Motion and Fugl-Meyer scale and FM Wrist-/Hand component. An increase in cortical-excitability in ipsilesional-hemisphere was found to be statistically significant (p < 0.05) in RG over CG, as indexed by a decrease in Resting Motor Threshold and increase in the amplitude of Motor Evoked Potential. No significant changes were shown by the contralesional-hemisphere. Interhemispheric RMT-asymmetry evidenced significant (p < 0.05) changes in RG over CG indicating increased cortical-excitability in ipsilesional-hemisphere along with interhemispheric changes.
Conclusion
Robotic-exoskeleton training showed improvement in motor outcomes and cortical-excitability in patients with stroke. Neurophysiological changes in RG could most likely be a consequence of plastic reorganization and use-dependent plasticity.
Trial registry number: ISRCTN95291802
Introduction
Stroke is one of the leading causes of mortality and morbidity worldwide [1]. Flexor hypertonia of the wrist is one of its common presentations. Post-stroke, the ability to actively initiate extension movement at the wrist and fingers is one of the indicators of the motor recovery [2, 3]. Regaining hand function and Activities of daily living (ADL) is particularly impervious to therapy owing to fine motor control needed for the distal-joints [4]. Conventional rehabilitation therapy is time taking, labor-intensive and subjective. Therapists usually have a high clinical load and a lack of evidence-based technologies to support them, resulting in therapist burnout and a healthcare system that cannot provide appropriate or effective rehabilitation services [5].
Although rehabilitation with neuro-rehabilitation robots has shown encouraging clinical results [5,6,7,8,9,10,11,12,13,14,15,16,17,18], it is currently limited to a very few hospitals and not widely used because of the associated high-cost and an infrastructural-requirement to station these large and complex devices with a high set-up time and limited usability [19,20,21]. Rehabilitation strategies need to take into account the multifaceted nature of the disability, which is self-changing (progressing or improving), i.e. itself changes with time and requires a multimodal approach. Hence, the assistive device needs to be flexible and adaptive enough to accommodate the needs of a large patient population.
An effective rehabilitation device for the upper-limb should be able to facilitate a specific pattern of coordinated movements of joints, especially for a hand. However, this particular coordination is currently not integrated with any of the commercially available devices, where they mostly focus on movements of the specific individual joint in isolation [22]. For a healthy subject, extending the wrist naturally leads to flexion of the fingers. Semi-extension of the wrist with grasped fingers contributes to ADL movements; which is also commonly disrupted in patients with stroke due to flexor hypertonia. These complex movement patterns have been disintegrated during conventional physiotherapy into few simpler tasks, for example, holding a glass of water consists of sub-tasks like grasping the glass with the fingers in the motion of flexion while wrist in 30–40 degree semi-extended position, and releasing it with fingers being in extension and wrist coming back to the neutral position with flexion as elaborated in [23]. Hence, a device that can simulate the movement pattern of wrist extension along with finger flexion (such as in ADL), maintaining inter-joint coordination with the limited number of actuators making the device less complex, is the need of the hour. Only two devices, Hand Mentor and HWARD, allow hand and wrist synchronization [24]. The Hand Mentor Pro rotates wrist with Metacarpophalengeal (MCP) placed at a constant angle with respect to the wrist, but lacks flexion (grasp) and extension (release) of MCP, also it can’t accommodate patient-centric ROM and speed. Though HWARD synchronized wrist and MCP and provided seminal evidence of reorganization of the brain through robotic-therapy sessions, it had few other challenges such as limited range of motion, no patient-centric muscle-specific training, finger opening requirement, manual adjustment of force at pneumatic cylinders and device having ~ 25 kg of weight. Hence, the challenges remained to simplify the complex design and therapy protocols into simple, lightweight, user-friendly devices that are convenient with a potential to use even in home-settings. Moreover, the device must show efficacy for a broader community while being cost-effective for low and middle-income countries with limited research on rehabilitation [25,26,27]. Our device attempt to address the key limitations which other commercial devices faced.
In our previous work, we have designed a robotic hand exoskeleton for rehabilitation of the wrist and MCP joint, to synchronize wrist extension with finger-flexion and wrist-flexion with finger extension [28]. It is a prototype device with the potential of being simple and easy to operate exoskeleton rehabilitation device for low-resource settings in the future. The exoskeleton targets spasticity through a synergy-based rehabilitation approach while also maintaining patient-initiated therapy through residual muscle activity for maximizing voluntary effort. The lightweight and portable device indicated an improvement in quantitative motor clinical outcomes in patients with chronic stroke [28].
The aim of the present study was twofold. The first objective was to assess the clinical effectiveness of the novel robotic-exoskeleton device [28] and the second is a comparison of its clinical effectiveness with conventional upper-limb rehabilitation. There is a considerable amount of literature documented for neurorehabilitation robots that takes into account the specific, repetitive, and timed movement goals [29] with maximizing voluntary residual muscle activity, real-time visual performance biofeedback, and proprioceptive feedback for sensorimotor integration. These features might give the robotic-therapy a notch over dose-matched conventional therapy [30, 31]. As the exoskeleton device also has these features [28], thus, we hypothesized that exoskeleton-based rehabilitation therapy might also encourage clinically relevant neuroplasticity with expected better clinical outcomes for distal joints in patients with stroke than the dose-matched conventional rehabilitation.[…]
[Abstract] Evidence for a Window of Enhanced Plasticity in the Human Motor Cortex Following Ischemic Stroke
Posted by Kostas Pantremenos in Neuroplasticity on April 26, 2021
Abstract
Background
In preclinical models, behavioral training early after stroke produces larger gains compared with delayed training. The effects are thought to be mediated by increased and widespread reorganization of synaptic connections in the brain. It is viewed as a period of spontaneous biological recovery during which synaptic plasticity is increased.
Objective
To look for evidence of a similar change in synaptic plasticity in the human brain in the weeks and months after ischemic stroke.
Methods
We used continuous theta burst stimulation (cTBS) to activate synapses repeatedly in the motor cortex. This initiates early stages of synaptic plasticity that temporarily reduces cortical excitability and motor-evoked potential amplitude. Thus, the greater the effect of cTBS on the motor-evoked potential, the greater the inferred level of synaptic plasticity. Data were collected from separate cohorts (Australia and UK). In each cohort, serial measurements were made in the weeks to months following stroke. Data were obtained for the ipsilesional motor cortex in 31 stroke survivors (Australia, 66.6 ± 17.8 years) over 12 months and the contralesional motor cortex in 29 stroke survivors (UK, 68.2 ± 9.8 years) over 6 months.
Results
Depression of cortical excitability by cTBS was most prominent shortly after stroke in the contralesional hemisphere and diminished over subsequent sessions (P = .030). cTBS response did not differ across the 12-month follow-up period in the ipsilesional hemisphere (P = .903).
Conclusions
Our results provide the first neurophysiological evidence consistent with a period of enhanced synaptic plasticity in the human brain after stroke. Behavioral training given during this period may be especially effective in supporting poststroke recovery.
[ARTICLE] A novel glasses-free virtual reality rehabilitation system on improving upper limb motor function among patients with stroke: a feasibility pilot study – Full Text
Posted by Kostas Pantremenos in Paretic Hand, REHABILITATION, tDCS/rTMS, Virtual reality rehabilitation on April 9, 2021
Abstract
Background
Virtual reality (VR) technology is increasingly used in stroke rehabilitation. This study aimed to investigate the effectiveness of using the glasses-free VR training to improve motor function of upper limb in patients with stroke.
Methods
Twelve patients with stroke were recruited to participate in the intervention of 3 weeks. At the baseline and post intervention, two times of evaluation including Fugl-Meyer upper-extremity scale (FMS-UE), transcranial magnetic stimulation (TMS) measurement and motion evaluation were performed.
Results
No significant difference was observed between two groups at baseline evaluation. After the intervention, the FMS-UE scores presented a greater improvement in the VR group compared with the control group. TMS measurement showed that there was significant difference in cortex latency and central motor conduction time between two groups after the intervention, but no significant difference in the amplitude of motor event potential was observed. In addition, there was a significant correlation between game scores and FMS-UE scores.
Conclusions
The novel glasses-free VR training was at least as effective as conventional occupational therapy in upper limb motor function, improving nerve conduction time and corticospinal excitability in patient with stroke.
1. Introduction
Stroke is among the leading cause of long-term disability with up to 85% of patients with stroke experience upper limb motor deficits [1]. Motor function of upper limb, in particular the hand function, occupies more than 60% of the physical function for an individual [2]. However, the recovery of upper limb motor function post stroke is clinical challenging, and the outcomes of upper limb rehabilitation remains unsatisfactory [1]. The loss of control input from the brain is believed to be a contributor to muscle spasm and flaccid paresis, leading to the difficulty in performing daily activities and reduced quality of life among patients with stroke [3]. Additionally, early literature also suggested that there was a significant descending information flow which potentially reflected the recruitment of motor neurons from the supplementary motor area [4]. Thus, the recovery of the corticospinal pathway is likely to be a precondition of motor function improvement for patients with stroke [4,5].
Virtual reality (VR) technology has emerged as a promising intervention to facilitate functional recovery among patients with stroke [6]. VR intervention provides interactive tasks within a computer-generated virtual environment which incorporates auditory and visual feedback [7]. It has the advantage to increase users’ motivation by providing the high intensity repetitive tasks [8]. A previous review demonstrated the potential benefits of VR to improve upper limb function and activities of daily living (ADL) function in patients with stroke [9]. However, the clinical effectiveness of VR systems in the recovery of hand function remains unsatisfied [9]. The high complexity of the hand represents a challenge to accurately capture and simulate the movements of the hands and fingers [6,10,11].Thus, stroke patients could not obtain precise and timely feedback from the VR system, which contribute to poor clinical outcome [9,12]. Although gloves or other wearable devices with built-in motion sensors are often adopted in some VR systems to capture hand movements, these wearable items place extraneous load on the users which reduce motion velocity and increases the difficulty of training for patients with stroke [13,14]. Leap Motion© Controller (LMC) is a device designed to capture the fine motions of hands and fingers [6]. Compared with other devices, LMC has the benefits of low-cost and easiness to use [15]. To date, three studies were found that had trialed the LMC as part of a VR training system to capture hand movements in patients with stroke, and reported improvements in Wolf motor function test (WMFT) scores and performance time [6], higher hand abilities and grasp force [16], and increased Fugl-Meyer scale (FMS) scores and Box-and-Blocks Test scores [17]. These studies demonstrated the feasibility and potential benefits of LMC-based VR training in improving upper limb motor function among stroke patients. It should be noted that only a two-dimension (2D) display was used in those studies, which would not provide a stereoscopic virtual environment for patients with stroke.
The neurological mechanism of VR training to improve upper limb motor function in patients with stroke mainly involved two aspects, cortical reorganization [6] and the recovery of corticospinal tract [18]. Wang et al. [6] observed an increase in activation intensity from functional magnetic resonance imaging (fMRI) of the lesioned hemisphere in sub-acute stroke patients after four weeks of Leap Motion-based VR training. This finding provided support that Leap Motion-based VR intervention promote neuroplasticity which contribute to functional improvement [6,19].
The integrity of the corticospinal tract was demonstrated to be associated with motor function recovery in chronic stroke patients [20, 21]. A previous study suggested the positive relationship between the integrity of corticospinal tract and upper limb motor recovery in patients with cerebrovascular accidents [18]. Another research reported an improvement in the functional integrity of ipsilateral corticospinal tract and upper limb motor function after two weeks of VR training in patients with subacute stroke [22]. The author stated that stroke patients with higher motor evoked potentials (MEPs) had a significantly greater FMS and WMFT scores than those with MEP absence. It suggested that functional recovery of upper limb post stroke may be related to the ipsilesional corticospinal tract [22, 23]. However, there is still a lack of evidence whether neural conduction time would change after the VR training among stroke patients, and more research is needed.
Our institute has recently developed a novel glasses-free VR rehabilitation system that addressed the issues of external sensors to capture hands and finger motion of the existence VR system discussed above. This study was aimed to investigate whether the novel VR rehabilitation system was able to facilitate the recovery of upper limb motor function, as well as the corticospinal tract in patients with stroke. We hypothesized that after the glasses-free VR training, there would be an improvement in upper limb motor function and the function of corticospinal tract among patients with stroke.[…]

[Slideshow] Depression Overview: Emotional Symptoms, Physical Signs, and More
Posted by Kostas Pantremenos in Depression on February 4, 2021
Δημιουργήθηκε απόσπασμα από: https://www.webmd.com/depression/ss/slideshow-depression-overview
![passa]dap
passo]döa](https://tbirehabilitation.files.wordpress.com/2021/02/image.jpeg?w=493)
Depression: What Is It?
1 / 24
It’s natural to feel down sometimes, but if that low mood lingers day after day, it could signal depression. Major depression is an episode of sadness or apathy along with other symptoms that lasts at least two consecutive weeks and is severe enough to interrupt daily activities. Depression is not a sign of weakness or a negative personality. It is a major public health problem and a treatable medical condition.
Shown here are PET scans of the brain showing different activity levels in a person with depression, compared to a person without depression.

Depression Symptoms: Emotional
2 / 24
The primary symptoms of depression are a sad mood and/or loss of interest in life. Activities that were once pleasurable lose their appeal. Patients may also be haunted by a sense of guilt or worthlessness, lack of hope, and recurring thoughts of death or suicide.

Depression Symptoms: Physical
3 / 24
Depression is sometimes linked to physical symptoms. These include:
- Fatigue and decreased energy
- Insomnia, especially early-morning waking
- Excessive sleep
- Persistent aches or pains, headaches, cramps, or digestive problems that do not ease even with treatment
Depression can make other health problems feel worse, particularly chronic pain. Key brain chemicals influence both mood and pain. Treating depression has been shown to improve co-existing illnesses.

Depression Symptom: Appetite
4 / 24
Changes in appetite or weight are another hallmark of depression. Some patients develop increased appetite, while others lose their appetite altogether. Depressed people may experience serious weight loss or weight gain.

Impact on Daily Life
5 / 24
Without treatment, the physical and emotional turmoil brought on by depression can derail careers, hobbies, and relationships. People with depression often find it difficult to concentrate and make decisions. They turn away from previously enjoyable activities, including sex. In severe cases, depression can become life-threatening.

Suicide Warning Signs
6 / 24
People who are depressed are more likely to attempt suicide. Warning signs include talking about death or suicide, threatening to hurt people, or engaging in aggressive or risky behavior. Anyone who appears suicidal should be taken very seriously. Do not hesitate to call one of the suicide hotlines: 800-SUICIDE (800-784-2433) and 800-273-TALK (800-273-8255). If you have a plan to commit suicide, go to the emergency room for immediate treatment.

Depression: Who’s at Risk?
7 / 24
Anyone can become depressed, but many experts believe genetics play a role. Having a parent or sibling with depression increases your risk of developing the disorder. Women are twice as likely as men to become depressed.

Causes of Depression
8 / 24
Doctors aren’t sure what causes depression, but a prominent theory is altered brain structure and chemical function. Brain circuits that regulate mood may work less efficiently during depression. Drugs that treat depression are believed to improve communication between nerve cells, making them run more normally. Experts also think that while stress — such as losing a loved one — can trigger depression, one must first be biologically prone to develop the disorder. Other triggers could include certain medications, alcohol or substance abuse, hormonal changes, or even the season.
Illustrated here are neurons (nerve cells) in the brain communicating via neurotransmitters.

Seasonal Depression
9 / 24
If your mood matches the season — sunny in the summer, gloomy in the winter — you may have a form of depression called seasonal affective disorder (SAD). The onset of SAD usually occurs in the late fall and early winter, as the daylight hours grow shorter. Experts say SAD affects from 3% to 20% of all people, depending upon where they live.

Postpartum Depression
10 / 24
The “baby blues” strikes as many as three out of four new mothers. But nearly 12% develop a more intense dark mood that lingers even as their baby thrives. This is known as postpartum depression, and the symptoms are the same as those of major depression. An important difference is that the baby’s well-being is also at stake. A depressed mother may have trouble enjoying and bonding with their infant.

Depression in Children
11 / 24
In the United States, depression affects 2% of grade school kids and about one in 10 teenagers. It interferes with the ability to play, make friends, and complete schoolwork. Symptoms are similar to depression in adults, but some children may appear angry or engage in risky behavior, called “acting out.” Depression can be difficult to diagnose in children.

Diagnosing Depression
12 / 24
As of yet, there is no lab test for depression. To make an accurate diagnosis, doctors rely on a patient’s description of the symptoms. You’ll be asked about your medical history and medication use since these may contribute to symptoms of depression. Discussing moods, behaviors, and daily activities can help reveal the severity and type of depression. This is a critical step in determining the most effective treatment.

Talk Therapy for Depression
13 / 24
Studies suggest different types of talk therapy can fight mild to moderate depression. Cognitive behavioral therapy aims to change thoughts and behaviors that contribute to depression. Interpersonal therapy identifies how your relationships impact your mood. Psychodynamic psychotherapy helps people understand how their behavior and mood are affected by unresolved issues and unconscious feelings. Some patients find a few months of therapy are all they need, while others continue long term.

Medications for Depression
14 / 24
Antidepressants affect the levels of brain chemicals, such as serotonin and norepinephrine. There are many options. Give antidepressants a few weeks of use to take effect. Good follow-up with your doctor is important to evaluate their effectiveness and make dosage adjustments. If the first medication tried doesn’t help, there’s a good chance another will. The combination of talk therapy and medication appears particularly effective.

Exercise for Depression
15 / 24
Research suggests exercise is a potent weapon against mild to moderate depression. Physical activity releases endorphins that can help boost mood. Regular exercise is also linked to higher self-esteem, better sleep, less stress, and more energy. Any type of moderate activity, from swimming to housework, can help. Choose something you enjoy and aim for 20 to 30 minutes four or five times a week.

Light Therapy (Phototherapy)
16 / 24
Light therapy has shown promise as an effective treatment not only for SAD but for some other types of depression as well. It involves sitting in front of a specially designed light box that provides either a bright or dim light for a prescribed amount of time each day. Light therapy may be used in conjunction with other treatments. Talk to your doctor about getting a light box and the recommended length of time for its use.

St. John’s Wort for Depression
17 / 24
St. John’s wort is an herbal supplement that has been the subject of extensive debate. There is some evidence that it can fight mild depression, but two large studies have shown it is ineffective against moderately severe major depression. St. John’s wort can interact with other medications you may be taking for medical conditions or birth control. Talk to your doctor before taking this or any other supplement.

Pets for Depression
18 / 24
A playful puppy or wise-mouthed parrot is no substitute for medication or talk therapy. But researchers say pets can ease the symptoms of mild to moderate depression in many people. Pets provide unconditional love, relieve loneliness, and give patients a sense of purpose. Studies have found pet owners have less trouble sleeping and better overall health.

The Role of Social Support
19 / 24
Because loneliness goes hand-in-hand with depression, developing a social support network can be an important part of treatment. This may include joining a support group, finding an online support community, or making a genuine effort to see friends and family more often. Even joining a book club or taking classes at your gym can help you connect with people on a regular basis.

Vagus Nerve Stimulation (VNS)
20 / 24
Vagus nerve stimulation (VNS) may help patients with treatment-resistant depression that does not improve with medication. VNS is like a pacemaker for the brain. The surgically implanted device sends electrical pulses to the brain through the vagus nerve in the neck. These pulses are believed to ease depression by affecting mood areas of the brain.

Electroconvulsive Therapy (ECT)
21 / 24
Another option for patients with treatment-resistant or severe melancholic depression is electroconvulsive therapy (ECT). This treatment uses electric charges to create a controlled seizure. Patients are not conscious for the procedure. ECT helps 80% to 90% of patients who receive it, giving new hope to those who don’t improve with medication.

Transcranial Magnetic Stimulation
22 / 24
A newer option for people with stubborn depression is repetitive transcranial magnetic stimulation (rTMS). This treatment aims electromagnetic pulses at the skull. It stimulates a tiny electrical current in a part of the brain linked to depression. rTMS does not cause a seizure and appears to have few side effects. But doctors are still fine-tuning this treatment.

Good Outlook
23 / 24
In the midst of major depression, you may feel hopeless and helpless. But the fact is, this condition is highly treatable. More than 80% of people get better with medication, talk therapy, or a combination of the two. Even when these therapies fail to help, there are cutting-edge treatments that pick up the slack.
Sources Reviewed by Melinda Ratini, DO, MS on August 06, 2020
IMAGES PROVIDED BY:
(1) Science Source / Photo Researchers, Inc.
(2) Glowimages
(3) Bartomeu Amengual / age fotostock
(4) Jutta Klee / Stone
(5) Symphonie / Iconica
(6) Nikolaevich / Photonica
(7) Jetta Productions, Inc / Iconica
(8) 3D4Medical.com
(9) Megan Wyeth / Aurora
(10) Charles Gullung / Photonica
(11) Image Source
(12) Steve McAlister / Riser
(13) Mauro Fermariello / Photo Researchers, Inc.
(14) Mauro Fermariello / Photo Researchers, Inc.
(15) Katzer / Mauritius
(16) Christopher Furlong / Getty Images
(17) Dr. Jeremy Burgess / Photo Researchers, Inc.
(18) Leigh Schindler / Photodisc
(19) Alistair Berg / Digital Vision
(20) David J. Phillip / AP
(21) Will McIntyre / Photo Researchers, Inc.
(22) Universal Images Group / Getty
(23) Frank Gaglione / Riser
SOURCES:
Barkham, M. British Medical Bulletin, 2001.
Gjerdinjen, D. Journal of the American Board of Family Medicine, 2007.
Harvard Health Publications: “Exercise and Depression.”
Johns Hopkins Health Alerts: “The Many Benefits of Pets.”
Johns Hopkins Medicine: “Seasonal Affective Disorder.”
Mental Health America: “Co-occuring Disorders and Depression.”
National Institute of Mental Health, National Institutes of Health: “How is depression diagnosed and treated?” “What causes depression?” “What are the signs and symptoms of depression?” “What illnesses often co-exist with depression?” “Magnetic Stimulation Scores Modest Success as Antidepressant,” “Major Depressive Disorder in Children.”
The Merck Manual: “Depression.”
This tool does not provide medical advice. See additional information.
[Abstract + References] Canadian Platform for Trials in Noninvasive Brain Stimulation (CanStim) Consensus Recommendations for Repetitive Transcranial Magnetic Stimulation in Upper Extremity Motor Stroke Rehabilitation Trials
Posted by Kostas Pantremenos in Paretic Hand, tDCS/rTMS on January 12, 2021
Abstract
Objective. To develop consensus recommendations for the use of repetitive transcranial magnetic stimulation (rTMS) as an adjunct intervention for upper extremity motor recovery in stroke rehabilitation clinical trials.
Participants. The Canadian Platform for Trials in Non-Invasive Brain Stimulation (CanStim) convened a multidisciplinary team of clinicians and researchers from institutions across Canada to form the CanStim Consensus Expert Working Group.
Consensus Process. Four consensus themes were identified: (1) patient population, (2) rehabilitation interventions, (3) outcome measures, and (4) stimulation parameters. Theme leaders conducted comprehensive evidence reviews for each theme, and during a 2-day Consensus Meeting, the Expert Working Group used a weighted dot-voting consensus procedure to achieve consensus on recommendations for the use of rTMS as an adjunct intervention in motor stroke recovery rehabilitation clinical trials.
Results. Based on best available evidence, consensus was achieved for recommendations identifying the target poststroke population, rehabilitation intervention, objective and subjective outcomes, and specific rTMS parameters for rehabilitation trials evaluating the efficacy of rTMS as an adjunct therapy for upper extremity motor stroke recovery.
Conclusions. The establishment of the CanStim platform and development of these consensus recommendations is a first step toward the translation of noninvasive brain stimulation technologies from the laboratory to clinic to enhance stroke recovery.
References
| 1. | Veerbeek, JM, van Wegen, E, van Peppen, R, et al. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS One. 2014;9:e87987. Google Scholar | Crossref | Medline | ISI |
| 2. | Boyd, LA, Vidoni, ED, Wessel, BD. Motor learning after stroke: is skill acquisition a prerequisite for contralesional neuroplastic change? Neurosci Lett. 2010;482:21-25. Google Scholar | Crossref | Medline | ISI |
| 3. | Dimyan, MA, Cohen, LG. Neuroplasticity in the context of motor rehabilitation after stroke. Nat Rev Neurol. 2011;7:76-85. Google Scholar | Crossref | Medline | ISI |
| 4. | Arya, KN, Verma, R, Garg, RK, Sharma, VP, Agarwal, M, Aggarwal, GG. Meaningful task-specific training (MTST) for stroke rehabilitation: a randomized controlled trial. Top Stroke Rehabil. 2012;19:193-211. Google Scholar | Crossref | Medline | ISI |
| 5. | French, B, Thomas, LH, Coupe, J, et al. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst Rev. 2016;(11):CD006073. Google Scholar | Medline |
| 6. | Kimberley, TJ, Samargia, S, Moore, LG, Shakya, JK, Lang, CE. Comparison of amounts and types of practice during rehabilitation for traumatic brain injury and stroke. J Rehabil Res Dev. 2010;47:851-862. Google Scholar | Crossref | Medline |
| 7. | Teasell, R, Meyer, MJ, Foley, N, Salter, K, Willems, D. Stroke rehabilitation in Canada: a work in progress. Top Stroke Rehabil. 2009;16:11-19. Google Scholar | Crossref | Medline | ISI |
| 8. | Barrett, M, Snow, JC, Kirkland, MC, et al. Excessive sedentary time during in-patient stroke rehabilitation. Top Stroke Rehabil. 2018;25:366-374. Google Scholar | Medline |
| 9. | Rossi, S, Hallett, M, Rossini, PM, Pascual-Leone, A; Safety of TMS Consensus Group . Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol. 2009;120:2008-2039. Google Scholar | Crossref | Medline | ISI |
| 10. | Koganemaru, S, Mima, T, Thabit, MN, et al. Recovery of upper-limb function due to enhanced use-dependent plasticity in chronic stroke patients. Brain. 2010;133:3373-3384. Google Scholar | Crossref | Medline |
| 11. | Corti, M, Patten, C, Triggs, W. Repetitive transcranial magnetic stimulation of motor cortex after stroke: a focused review. Am J Phys Med Rehabil. 2012;91:254-270. Google Scholar | Crossref | Medline | ISI |
| 12. | Pascual-Leone, A, Pridmore, H. Transcranial magnetic stimulation (TMS). Aust N Z J Psychiatry. 1995;29:698. Google Scholar | Medline |
| 13. | Di Lazzaro, V, Rothwell, JC. Corticospinal activity evoked and modulated by non-invasive stimulation of the intact human motor cortex. J Physiol. 2014;592:4115-4128. Google Scholar | Crossref | Medline | ISI |
| 14. | Di Lazzaro, V, Dileone, M, Pilato, F, et al. Modulation of motor cortex neuronal networks by rTMS: comparison of local and remote effects of six different protocols of stimulation. J Neurophysiol. 2011;105:2150-2156. Google Scholar | Crossref | Medline | ISI |
| 15. | Hamada, M, Hanajima, R, Terao, Y, et al. Origin of facilitation in repetitive, 1.5 ms interval, paired pulse transcranial magnetic stimulation (rPPS) of the human motor cortex. Clin Neurophysiol. 2007;118:1596-1601. Google Scholar | Crossref | Medline |
| 16. | Takeuchi, N, Chuma, T, Matsuo, Y, Watanabe, I, Ikoma, K. Repetitive transcranial magnetic stimulation of contralesional primary motor cortex improves hand function after stroke. Stroke. 2005;36:2681-2686. Google Scholar | Crossref | Medline | ISI |
| 17. | van Lieshout, ECC, Visser-Meily, JMA, Neggers, SFW, van der Worp, HB, Dijkhuizen, RM. Brain stimulation for arm recovery after stroke (B-STARS): protocol for a randomised controlled trial in subacute stroke patients. BMJ Open. 2017;7:e016566. Google Scholar | Crossref | Medline |
| 18. | Thiel, A, Black, SE, Rochon, EA, et al. Non-invasive repeated therapeutic stimulation for aphasia recovery: a multilingual, multicenter aphasia trial. J Stroke Cerebrovasc Dis. 2015;24:751-758. Google Scholar | Crossref | Medline |
| 19. | Harvey, RL, Edwards, D, Dunning, K, et al. Randomized sham-controlled trial of navigated repetitive transcranial magnetic stimulation for motor recovery in stroke. Stroke. 2018;49:2138-2146. Google Scholar | Crossref | Medline |
| 20. | Lefaucheur, JP, Aleman, A, Baeken, C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014-2018). Clin Neurophysiol. 2020;131:474-528. Google Scholar | Crossref | Medline |
| 21. | Kwakkel, G, Lannin, NA, Borschmann, K, et al. Standardized measurement of sensorimotor recovery in stroke trials: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke. 2017;12:451-461. Google Scholar | SAGE Journals | ISI |
| 22. | Pollock, A, Farmer, SE, Brady, MC, et al. Interventions for improving upper limb function after stroke. Cochrane Database Syst Rev. 2014;2014(11):CD010820. Google Scholar |
| 23. | Coupar, F, Pollock, A, Rowe, P, Weir, C, Langhorne, P. Predictors of upper limb recovery after stroke: a systematic review and meta-analysis. Clin Rehabil. 2012;26:291-313. Google Scholar | SAGE Journals | ISI |
| 24. | Hatem, SM, Saussez, G, Della Faille, M, et al. Rehabilitation of motor function after stroke: a multiple systematic review focused on techniques to stimulate upper extremity recovery. Front Hum Neurosci. 2016;10:442. Google Scholar | Crossref | Medline |
| 25. | Hao, Z, Wang, D, Zeng, Y, Liu, M. Repetitive transcranial magnetic stimulation for improving function after stroke. Cochrane Database Syst Rev. 2013;(5):CD008862. Google Scholar | Medline |
| 26. | Sebastianelli, L, Versace, V, Martignago, S, et al. Low-frequency rTMS of the unaffected hemisphere in stroke patients: a systematic review. Acta Neurol Scand. 2017;136:585-605. Google Scholar | Crossref | Medline |
| 27. | Hsu, WY, Cheng, CH, Liao, KK, Lee, IH, Lin, YY. Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke. 2012;43:1849-1857. Google Scholar | Crossref | Medline | ISI |
| 28. | Paolucci, S, Antonucci, G, Grasso, MG, et al. Early versus delayed inpatient stroke rehabilitation: a matched comparison conducted in Italy. Arch Phys Med Rehabil. 2000;81:695-700. Google Scholar | Crossref | Medline | ISI |
| 29. | Jorgensen, HS, Nakayama, H, Raaschou, HO, Vive-Larsen, J, Stoier, M, Olsen, TS. Outcome and time course of recovery in stroke. Part II: time course of recovery. The Copenhagen Stroke Study. Arch Phys Med Rehabil. 1995;76:406-412. Google Scholar | Crossref | Medline | ISI |
| 30. | Hayward, KS, Schmidt, J, Lohse, KR, et al. Are we armed with the right data? Pooled individual data review of biomarkers in people with severe upper limb impairment after stroke. Neuroimage Clin. 2017;13:310-319. Google Scholar | Crossref | Medline |
| 31. | Bembenek, JP, Kurczych, K, KarliNski, M, Czlonkowska, A. The prognostic value of motor-evoked potentials in motor recovery and functional outcome after stroke—a systematic review of the literature. Funct Neurol. 2012;27:79-84. Google Scholar | Medline | ISI |
| 32. | Boyd, LA, Hayward, KS, Ward, NS, et al. Biomarkers of stroke recovery: Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke. 2017;12:480-493. Google Scholar | SAGE Journals | ISI |
| 33. | Langhorne, P, Bernhardt, J, Kwakkel, G. Stroke rehabilitation. Lancet. 2011;377:1693-1702. Google Scholar | Crossref | Medline | ISI |
| 34. | Zhang, L, Xing, G, Fan, Y, Guo, Z, Chen, H, Mu, Q. Short- and long-term effects of repetitive transcranial magnetic stimulation on upper limb motor function after stroke: a systematic review and meta-analysis. Clin Rehabil. 2017;31:1137-1153. Google Scholar | SAGE Journals | ISI |
| 35. | Xiang, H, Sun, J, Tang, X, Zeng, K, Wu, X. The effect and optimal parameters of repetitive transcranial magnetic stimulation on motor recovery in stroke patients: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil. 2019;33:847-864. Google Scholar | SAGE Journals | ISI |
| 36. | O’Brien, AT, Bertolucci, F, Torrealba-Acosta, G, Huerta, R, Fregni, F, Thibaut, A. Non-invasive brain stimulation for fine motor improvement after stroke: a meta-analysis. Eur J Neurol. 2018;25:1017-1026. Google Scholar | Crossref | Medline |
| 37. | Farmer, SE, Durairaj, V, Swain, I, Pandyan, AD. Assistive technologies: can they contribute to rehabilitation of the upper limb after stroke? Arch Phys Med Rehabil. 2014;95:968-985. Google Scholar | Crossref | Medline | ISI |
| 38. | Agosta, S, Galante, E, Ferraro, F, Pascual-Leone, A, Oster, J, Battelli, L. Report of a delayed seizure after low frequency repetitive transcranial magnetic stimulation in a chronic stroke patient. Clin Neurophysiol. 2016;127:1736-1737. Google Scholar | Crossref | Medline |
| 39. | Kumar, N, Padma Srivastava, MV, Verma, R, Sharma, H, Modak, T. Can low-frequency repetitive transcranial magnetic stimulation precipitate a late-onset seizure in a stroke patient? Clin Neurophysiol. 2016;127:1734-1736. Google Scholar | Crossref | Medline |
| 40. | Liepert, J, Zittel, S, Weiller, C. Improvement of dexterity by single session low-frequency repetitive transcranial magnetic stimulation over the contralesional motor cortex in acute stroke: a double-blind placebo-controlled crossover trial. Restor Neurol Neurosci. 2007;25:461-465. Google Scholar | Medline | ISI |
| 41. | Nitsche, MA . Co-incidence or causality? Seizures after slow rTMS in stroke patients. Clin Neurophysiol. 2016;127:1020-1021. Google Scholar | Crossref | Medline |
| 42. | Lefaucheur, JP, Andre-Obadia, N, Antal, A, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin Neurophysiol. 2014;125:2150-2206. Google Scholar | Crossref | Medline | ISI |
| 43. | Ameli, M, Grefkes, C, Kemper, F, et al. Differential effects of high-frequency repetitive transcranial magnetic stimulation over ipsilesional primary motor cortex in cortical and subcortical middle cerebral artery stroke. Ann Neurol. 2009;66:298-309. Google Scholar | Crossref | Medline | ISI |
| 44. | Park, CH, Kou, N, Ward, NS. The contribution of lesion location to upper limb deficit after stroke. J Neurol Neurosurg Psychiatry. 2016;87:1283-1286. Google Scholar | Crossref | Medline | ISI |
| 45. | Parikh, RM, Robinson, RG, Lipsey, JR, Starkstein, SE, Fedoroff, JP, Price, TR. The impact of poststroke depression on recovery in activities of daily living over a 2-year follow-up. Arch Neurol. 1990;47:785-789. Google Scholar | Crossref | Medline |
| 46. | MacIntosh, BJ, Edwards, JD, Kang, M, et al. Post-stroke fatigue and depressive symptoms are differentially related to mobility and cognitive performance. Front Aging Neurosci. 2017;9:343. Google Scholar | Crossref | Medline |
| 47. | Ginex, V, Veronelli, L, Vanacore, N, Lacorte, E, Monti, A, Corbo, M. Motor recovery in post-stroke patients with aphasia: the role of specific linguistic abilities. Top Stroke Rehabil. 2017;24:428-434. Google Scholar | Crossref | Medline |
| 48. | Cunningham, DA, Machado, A, Janini, D, et al. Assessment of inter-hemispheric imbalance using imaging and noninvasive brain stimulation in patients with chronic stroke. Arch Phys Med Rehabil. 2015;96(4 suppl):S94-S103. Google Scholar | Crossref | Medline |
| 49. | Casaubon, LK, Boulanger, JM, Glasser, E, et al. Canadian Stroke Best Practice Recommendations: acute inpatient stroke care guidelines, update 2015. Int J Stroke. 2016;11:239-252. Google Scholar | SAGE Journals | ISI |
| 50. | Teasell, R, Norine, F, Richardson, M, Allen, L, Cotoi, A. Outpatient Stroke Rehabilitation 2018. Accessed December 7, 2020. http://www.ebrsr.com/ Google Scholar |
| 51. | Peurala, SH, Kantanen, MP, Sjogren, T, Paltamaa, J, Karhula, M, Heinonen, A. Effectiveness of constraint-induced movement therapy on activity and participation after stroke: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil. 2012;26:209-223. Google Scholar | SAGE Journals | ISI |
| 52. | Hubbard, IJ, Parsons, MW, Neilson, C, Carey, LM. Task-specific training: evidence for and translation to clinical practice. Occup Ther Int. 2009;16:175-189. Google Scholar | Crossref | Medline | ISI |
| 53. | Wattchow, KA, McDonnell, MN, Hillier, SL. Rehabilitation interventions for upper limb function in the first four weeks following stroke: a systematic review and meta-analysis of the evidence. Arch Phys Med Rehabil. 2018;99:367-382. Google Scholar | Crossref | Medline |
| 54. | Waddell, KJ, Birkenmeier, RL, Moore, JL, Hornby, TG, Lang, CE. Feasibility of high-repetition, task-specific training for individuals with upper-extremity paresis. Am J Occup Ther. 2014;68:444-453. Google Scholar | Crossref | Medline | ISI |
| 55. | Almhdawi, KA, Mathiowetz, VG, White, M, delMas, RC. Efficacy of occupational therapy task-oriented approach in upper extremity post-stroke rehabilitation. Occup Ther Int. 2016;23:444-456. Google Scholar | Crossref | Medline |
| 56. | Askim, T, Indredavik, B, Vangberg, T, Haberg, A. Motor network changes associated with successful motor skill relearning after acute ischemic stroke: a longitudinal functional magnetic resonance imaging study. Neurorehabil Neural Repair. 2009;23:295-304. Google Scholar | SAGE Journals | ISI |
| 57. | Hebert, D, Lindsay, MP, McIntyre, A, et al. Canadian stroke best practice recommendations: stroke rehabilitation practice guidelines, update 2015. Int J Stroke. 2016;11:459-484. Google Scholar | SAGE Journals | ISI |
| 58. | Kunkel, A, Kopp, B, Muller, G, et al. Constraint-induced movement therapy for motor recovery in chronic stroke patients. Arch Phys Med Rehabil. 1999;80:624-628. Google Scholar | Crossref | Medline | ISI |
| 59. | Harris, JE, Eng, JJ, Miller, WC, Dawson, AS. A self-administered Graded Repetitive Arm Supplementary Program (GRASP) improves arm function during inpatient stroke rehabilitation: a multi-site randomized controlled trial. Stroke. 2009;40:2123-2128. Google Scholar | Crossref | Medline | ISI |
| 60. | Thrane, G, Friborg, O, Anke, A, Indredavik, B. A meta-analysis of constraint-induced movement therapy after stroke. J Rehabil Med. 2014;46:833-842. Google Scholar | Crossref | Medline |
| 61. | Pedlow, K, Lennon, S, Wilson, C. Application of constraint-induced movement therapy in clinical practice: an online survey. Arch Phys Med Rehabil. 2014;95:276-282. Google Scholar | Crossref | Medline |
| 62. | Viana, R, Teasell, R. Barriers to the implementation of constraint-induced movement therapy into practice. Top Stroke Rehabil. 2012;19:104-114. Google Scholar | Crossref | Medline | ISI |
| 63. | Fleet, A, Che, M, Mackay-Lyons, M, et al. Examining the use of constraint-induced movement therapy in Canadian neurological occupational and physical therapy. Physiother Can. 2014;66:60-71. Google Scholar | Crossref | Medline |
| 64. | Connell, LA, McMahon, NE, Harris, JE, Watkins, CL, Eng, JJ. A formative evaluation of the implementation of an upper limb stroke rehabilitation intervention in clinical practice: a qualitative interview study. Implement Sci. 2014;9:90. Google Scholar | Crossref | Medline |
| 65. | Hiscock, A, Miller, S, Rothwell, J, Tallis, RC, Pomeroy, VM. Informing dose-finding studies of repetitive transcranial magnetic stimulation to enhance motor function: a qualitative systematic review. Neurorehabil Neural Repair. 2008;22:228-249. Google Scholar | SAGE Journals | ISI |
| 66. | Graef, P, Dadalt, MLR, Rodrigues, D, Stein, C, Pagnussat, AS. Transcranial magnetic stimulation combined with upper-limb training for improving function after stroke: a systematic review and meta-analysis. J Neurol Sci. 2016;369:149-158. Google Scholar | Crossref | Medline |
| 67. | Abo, M, Kakuda, W, Momosaki, R, et al. Randomized, multicenter, comparative study of NEURO versus CIMT in poststroke patients with upper limb hemiparesis: the NEURO-VERIFY Study. Int J Stroke. 2014;9:607-612. Google Scholar | SAGE Journals | ISI |
| 68. | Foley, N, McClure, JA, Meyer, M, Salter, K, Bureau, Y, Teasell, R. Inpatient rehabilitation following stroke: amount of therapy received and associations with functional recovery. Disabil Rehabil. 2012;34:2132-2138. Google Scholar | Crossref | Medline | ISI |
| 69. | Jette, DU, Latham, NK, Smout, RJ, Gassaway, J, Slavin, MD, Horn, SD. Physical therapy interventions for patients with stroke in inpatient rehabilitation facilities. Phys Ther. 2005;85:238-248. Google Scholar | Crossref | Medline | ISI |
| 70. | Hayward, KS, Brauer, SG. Dose of arm activity training during acute and subacute rehabilitation post stroke: a systematic review of the literature. Clin Rehabil. 2015;29:1234-1243. Google Scholar | SAGE Journals | ISI |
| 71. | Lohse, KR, Lang, CE, Boyd, LA. Is more better? Using metadata to explore dose-response relationships in stroke rehabilitation. Stroke. 2014;45:2053-2058. Google Scholar | Crossref | Medline | ISI |
| 72. | Lang, CE, Lohse, KR, Birkenmeier, RL. Dose and timing in neurorehabilitation: prescribing motor therapy after stroke. Curr Opin Neurol. 2015;28:549-555. Google Scholar | Crossref | Medline |
| 73. | Dromerick, AW, Lang, CE, Birkenmeier, RL, et al. Very early constraint-induced movement during stroke rehabilitation (VECTORS): a single-center RCT. Neurology. 2009;73:195-201. Google Scholar | Crossref | Medline | ISI |
| 74. | Santisteban, L, Teremetz, M, Bleton, JP, Baron, JC, Maier, MA, Lindberg, PG. Upper limb outcome measures used in stroke rehabilitation studies: a systematic literature review. PLoS One. 2016;11:e0154792. Google Scholar | Crossref | Medline | ISI |
| 75. | Hong, I, Bonilha, HS. Psychometric properties of upper extremity outcome measures validated by Rasch analysis: a systematic review. Int J Rehabil Res. 2017;40:1-10. Google Scholar | Crossref | Medline |
| 76. | Kirton, A, Chen, R, Friefeld, S, Gunraj, C, Pontigon, AM, Deveber, G. Contralesional repetitive transcranial magnetic stimulation for chronic hemiparesis in subcortical paediatric stroke: a randomised trial. Lancet Neurol. 2008;7:507-513. Google Scholar | Crossref | Medline | ISI |
| 77. | Noorkoiv, M, Rodgers, H, Price, CI. Accelerometer measurement of upper extremity movement after stroke: a systematic review of clinical studies. J Neuroeng Rehabil. 2014;11:144. Google Scholar | Crossref | Medline | ISI |
| 78. | Geyh, S, Kurt, T, Brockow, T, et al. Identifying the concepts contained in outcome measures of clinical trials on stroke using the International Classification of Functioning, Disability and Health as a reference. J Rehabil Med. 2004(44 suppl):56-62. Google Scholar | Crossref | Medline | ISI |
| 79. | Bushnell, C, Bettger, JP, Cockroft, KM, et al. Chronic stroke outcome measures for motor function intervention trials: expert panel recommendations. Circ Cardiovasc Qual Outcomes. 2015;8(6 suppl 3):S163-S169. Google Scholar | Crossref | Medline |
| 80. | Van der Lee, JH, De Groot, V, Beckerman, H, Wagenaar, RC, Lankhorst, GJ, Bouter, LM. The intra- and interrater reliability of the action research arm test: a practical test of upper extremity function in patients with stroke. Arch Phys Med Rehabil. 2001;82:14-19. Google Scholar | Crossref | Medline | ISI |
| 81. | Bonita, R, Beaglehole, R. Recovery of motor function after stroke. Stroke. 1988;19:1497-1500. Google Scholar | Crossref | Medline | ISI |
| 82. | Banks, JL, Marotta, CA. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38:1091-1096. Google Scholar | Crossref | Medline | ISI |
| 83. | Quinn, TJ, Dawson, J, Walters, MR, Lees, KR. Reliability of the modified Rankin Scale: a systematic review. Stroke. 2009;40:3393-3395. Google Scholar | Crossref | Medline | ISI |
| 84. | Pike, S, Lannin, NA, Wales, K, Cusick, A. A systematic review of the psychometric properties of the Action Research Arm Test in neurorehabilitation. Aust Occup Ther J. 2018;65:449-471. Google Scholar | Crossref | Medline |
| 85. | Alt Murphy, M, Resteghini, C, Feys, P, Lamers, I. An overview of systematic reviews on upper extremity outcome measures after stroke. BMC Neurol. 2015;15:29. Google Scholar | Crossref | Medline |
| 86. | Law, M, Baptiste, S, McColl, M, Opzoomer, A, Polatajko, H, Pollock, N. The Canadian Occupational Performance Measure: an outcome measure for occupational therapy. Can J Occup Ther. 1990;57:82-87. Google Scholar | SAGE Journals |
| 87. | Duncan, PW, Wallace, D, Lai, SM, Johnson, D, Embretson, S, Laster, LJ. The Stroke Impact Scale version 2.0. Evaluation of reliability, validity, and sensitivity to change. Stroke. 1999;30:2131-2140. Google Scholar | Crossref | Medline | ISI |
| 88. | Kirton, A, Ciechanski, P, Zewdie, E, et al. Transcranial direct current stimulation for children with perinatal stroke and hemiparesis. Neurology. 2017;88:259-267. Google Scholar | Crossref | Medline |
| 89. | Yang, SY, Lin, CY, Lee, YC, Chang, JH. The Canadian occupational performance measure for patients with stroke: a systematic review. J Phys Ther Sci. 2017;29:548-555. Google Scholar | Crossref | Medline |
| 90. | Katzan, IL, Thompson, NR, Lapin, B, Uchino, K. Added value of patient-reported outcome measures in stroke clinical practice. J Am Heart Assoc. 2017;6:e005356. Google Scholar | Crossref | Medline |
| 91. | Stewart, JC, Cramer, SC. Patient-reported measures provide unique insights into motor function after stroke. Stroke. 2013;44:1111-1116. Google Scholar | Crossref | Medline | ISI |
| 92. | Sullivan, JE, Espe, LE, Kelly, AM, Veilbig, LE, Kwasny, MJ. Feasibility and outcomes of a community-based, pedometer-monitored walking program in chronic stroke: a pilot study. Top Stroke Rehabil. 2014;21:101-110. Google Scholar | Crossref | Medline |
| 93. | Vetrovsky, T, Cupka, J, Dudek, M, et al. A pedometer-based walking intervention with and without email counseling in general practice: a pilot randomized controlled trial. BMC Public Health. 2018;18:635. Google Scholar | Crossref | Medline |
| 94. | Zhang, L, Xing, G, Shuai, S, et al. Low-frequency repetitive transcranial magnetic stimulation for stroke-induced upper limb motor deficit: a meta-analysis. Neural Plast. 2017;2017:2758097. Google Scholar | Crossref | Medline |
| 95. | Rossini, PM, Burke, D, Chen, R, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin Neurophysiol. 2015;126:1071-1107. Google Scholar | Crossref | Medline | ISI |
| 96. | Le, Q, Qu, Y, Tao, Y, Zhu, S. Effects of repetitive transcranial magnetic stimulation on hand function recovery and excitability of the motor cortex after stroke: a meta-analysis. Am J Phys Med Rehabil. 2014;93:422-430. Google Scholar | Crossref | Medline |
| 97. | Ludemann-Podubecka, J, Bosl, K, Nowak, DA. Repetitive transcranial magnetic stimulation for motor recovery of the upper limb after stroke. Prog Brain Res. 2015;218:281-311. Google Scholar | Crossref | Medline |
| 98. | Liepert, J, Restemeyer, C, Kucinski, T, Zittel, S, Weiller, C. Motor strokes: the lesion location determines motor excitability changes. Stroke. 2005;36:2648-2653. Google Scholar | Crossref | Medline | ISI |
| 99. | Shimizu, T, Hosaki, A, Hino, T, et al. Motor cortical disinhibition in the unaffected hemisphere after unilateral cortical stroke. Brain. 2002;125(pt 8):1896-1907. Google Scholar | Crossref | Medline | ISI |
| 100. | Volz, LJ, Vollmer, M, Michely, J, Fink, GR, Rothwell, JC, Grefkes, C. Time-dependent functional role of the contralesional motor cortex after stroke. Neuroimage Clin. 2017;16:165-174. Google Scholar | Crossref | Medline |
| 101. | Khedr, EM, Abdel-Fadeil, MR, Farghali, A, Qaid, M. Role of 1 and 3 Hz repetitive transcranial magnetic stimulation on motor function recovery after acute ischaemic stroke. Eur J Neurol. 2009;16:1323-1330. Google Scholar | Crossref | Medline | ISI |
| 102. | Sasaki, N, Mizutani, S, Kakuda, W, Abo, M. Comparison of the effects of high- and low-frequency repetitive transcranial magnetic stimulation on upper limb hemiparesis in the early phase of stroke. J Stroke Cerebrovasc Dis. 2013;22:413-418. Google Scholar | Crossref | Medline | ISI |
| 103. | Seniow, J, Bilik, M, Lesniak, M, Waldowski, K, Iwanski, S, Czlonkowska, A. Transcranial magnetic stimulation combined with physiotherapy in rehabilitation of poststroke hemiparesis: a randomized, double-blind, placebo-controlled study. Neurorehabil Neural Repair. 2012;26:1072-1079. Google Scholar | SAGE Journals | ISI |
| 104. | Etoh, S, Noma, T, Ikeda, K, et al. Effects of repetitive transcranial magnetic stimulation on repetitive facilitation exercises of the hemiplegic hand in chronic stroke patients. J Rehabil Med. 2013;45:843-847. Google Scholar | Crossref | Medline |
| 105. | Avenanti, A, Coccia, M, Ladavas, E, Provinciali, L, Ceravolo, MG. Low-frequency rTMS promotes use-dependent motor plasticity in chronic stroke: a randomized trial. Neurology. 2012;78:256-264. Google Scholar | Crossref | Medline | ISI |
| 106. | Fregni, F, Boggio, PS, Valle, AC, et al. A sham-controlled trial of a 5-day course of repetitive transcranial magnetic stimulation of the unaffected hemisphere in stroke patients. Stroke. 2006;37:2115-2122. Google Scholar | Crossref | Medline | ISI |
| 107. | Emara, TH, Moustafa, RR, Elnahas, NM, et al. Repetitive transcranial magnetic stimulation at 1 Hz and 5 Hz produces sustained improvement in motor function and disability after ischaemic stroke. Eur J Neurol. 2010;17:1203-1209. Google Scholar | Crossref | Medline | ISI |
| 108. | Takeuchi, N, Tada, T, Toshima, M, Matsuo, Y, Ikoma, K. Repetitive transcranial magnetic stimulation over bilateral hemispheres enhances motor function and training effect of paretic hand in patients after stroke. J Rehabil Med. 2009;41:1049-1054. Google Scholar | Crossref | Medline | ISI |
| 109. | Conforto, AB, Anjos, SM, Saposnik, G, et al. Transcranial magnetic stimulation in mild to severe hemiparesis early after stroke: a proof of principle and novel approach to improve motor function. J Neurol. 2012;259:1399-1405. Google Scholar | Crossref | Medline | ISI |
| 110. | Park, E, Kim, YH, Chang, WH, Kwon, TG, Shin, YI. Interhemispheric modulation of dual-mode, noninvasive brain stimulation on motor function. Ann Rehabil Med. 2014;38:297-303. Google Scholar | Crossref | Medline |
| 111. | Malcolm, MP, Triggs, WJ, Light, KE, et al. Repetitive transcranial magnetic stimulation as an adjunct to constraint-induced therapy: an exploratory randomized controlled trial. Am J Phys Med Rehabil. 2007;86:707-715. Google Scholar | Crossref | Medline | ISI |
| 112. | Wassermann, EM . Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5-7, 1996. Electroencephalogr Clin Neurophysiol. 1998;108:1-16. Google Scholar | Crossref | Medline |
| 113. | Muellbacher, W, Ziemann, U, Boroojerdi, B, Hallett, M. Effects of low-frequency transcranial magnetic stimulation on motor excitability and basic motor behavior. Clin Neurophysiol. 2000;111(6):1002-1007. Google Scholar | Crossref | Medline |
| 114. | Houdayer, E, Degardin, A, Cassim, F, Bocquillon, P, Derambure, P, Devanne, H. The effects of low- and high-frequency repetitive TMS on the input/output properties of the human corticospinal pathway. Exp Brain Res. 2008;187:207-217. Google Scholar | Crossref | Medline |
| 115. | Heide, G, Witte, OW, Ziemann, U. Physiology of modulation of motor cortex excitability by low-frequency suprathreshold repetitive transcranial magnetic stimulation. Exp Brain Res. 2006;171:26-34. Google Scholar | Crossref | Medline | ISI |
| 116. | de Jesus, DR, Favalli, GP, Hoppenbrouwers, SS, et al. Determining optimal rTMS parameters through changes in cortical inhibition. Clin Neurophysiol. 2014;125:755-762. Google Scholar | Crossref | Medline | ISI |
| 117. | Kantak, SS, Fisher, BE, Sullivan, KJ, Winstein, CJ. Effects of different doses of low frequency rTMS on motor corticospinal excitability. J Neurol Neurophysiol. 2010; 1:1000102. doi:10.4172/2155-9562.1000102 Google Scholar | Crossref |
| 118. | Pascual-Leone, A, Cohen, LG, Hallett, M. Cortical map plasticity in humans. Trends Neurosci. 1992;15:13-14. Google Scholar | Crossref | Medline |
| 119. | Liepert, J, Storch, P, Fritsch, A, Weiller, C. Motor cortex disinhibition in acute stroke. Clin Neurophysiol. 2000;111:671-676. Google Scholar | Crossref | Medline | ISI |
| 120. | Siebner, HR, Rothwell, J. Transcranial magnetic stimulation: new insights into representational cortical plasticity. Exp Brain Res. 2003;148:1-16. Google Scholar | Crossref | Medline | ISI |
| 121. | Ahdab, R, Ayache, SS, Brugieres, P, Farhat, WH, Lefaucheur, JP. The hand motor hotspot is not always located in the hand knob: a neuronavigated transcranial magnetic stimulation study. Brain Topogr. 2016;29:590-597. Google Scholar | Crossref | Medline |
| 122. | Liao, WW, Whitall, J, Wittenberg, GF, Barton, JE, McCombe Waller, S. Not all brain regions are created equal for improving bimanual coordination in individuals with chronic stroke. Clin Neurophysiol. 2019;130:1218-1230. Google Scholar | Crossref | Medline |
| 123. | Julkunen, P, Saisanen, L, Danner, N, et al. Comparison of navigated and non-navigated transcranial magnetic stimulation for motor cortex mapping, motor threshold and motor evoked potentials. Neuroimage. 2009;44:790-795. Google Scholar | Crossref | Medline | ISI |
| 124. | Saisanen, L, Julkunen, P, Niskanen, E, et al. Motor potentials evoked by navigated transcranial magnetic stimulation in healthy subjects. J Clin Neurophysiol. 2008;25:367-372. Google Scholar | Crossref | Medline | ISI |
| 125. | Sparing, R, Buelte, D, Meister, IG, Paus, T, Fink, GR. Transcranial magnetic stimulation and the challenge of coil placement: a comparison of conventional and stereotaxic neuronavigational strategies. Hum Brain Mapp. 2008;29:82-96. Google Scholar | Crossref | Medline | ISI |
| 126. | Cincotta, M, Giovannelli, F, Borgheresi, A, et al. Optically tracked neuronavigation increases the stability of hand-held focal coil positioning: evidence from “transcranial” magnetic stimulation-induced electrical field measurements. Brain Stimul. 2010;3:119-123. Google Scholar | Crossref | Medline |
[ARTICLE] Novel TMS for Stroke and Depression (NoTSAD): Accelerated Repetitive Transcranial Magnetic Stimulation as a Safe and Effective Treatment for Post-stroke Depression – Full Text
Posted by Kostas Pantremenos in Depression, tDCS/rTMS on November 16, 2020
Background: Post-stroke depression (PSD) affects up to 50% of stroke survivors, reducing quality of life, and increasing adverse outcomes. Conventional therapies to treat PSD may not be effective for some patients. Repetitive transcranial magnetic stimulation (rTMS) is well-established as an effective treatment for Major Depressive Disorder (MDD) and some small trials have shown that rTMS may be effective for chronic PSD; however, no trials have evaluated an accelerated rTMS protocol in a subacute stroke population. We hypothesized that an accelerated rTMS protocol will be a safe and viable option to treat PSD symptoms.
Methods: Patients (N = 6) with radiographic evidence of ischemic stroke within the last 2 weeks to 6 months with Hamilton Depression Rating Scale (HAMD-17) scores >7 were recruited for an open label study using an accelerated rTMS protocol as follows: High-frequency (20-Hz) rTMS at 110% resting motor threshold (RMT) was applied to the left dorsolateral prefrontal cortex (DLPFC) during five sessions per day over four consecutive days for a total of 20 sessions. Safety assessment and adverse events were documented based on the patients’ responses following each day of stimulation. Before and after the 4-days neurostimulation protocol, outcome measures were obtained for the HAMD, modified Rankin Scale (mRS), functional independence measures (FIM), and National Institutes of Health Stroke Scales (NIHSS). These same measures were obtained at 3-months follow up.
Results: HAMD significantly decreased (Wilcoxon p = 0.03) from M = 15.5 (2.81)−4.17 (0.98) following rTMS, a difference which persisted at the 3-months follow-up (p = 0.03). No statistically significant difference in FIM, mRS, or NIHSS were observed. No significant adverse events related to the treatment were observed and patients tolerated the stimulation protocol well overall.
Conclusions: This pilot study indicates that an accelerated rTMS protocol is a safe and viable option, and may be an effective alternative or adjunctive therapy for patients suffering from PSD. Future randomized, controlled studies are needed to confirm these preliminary findings.
Clinical Trial Registration: https://clinicaltrials.gov/ct2/show/NCT04093843.
Introduction
The interplay between depression and cerebrovascular disease is complex and clinically important. Post-stroke depression (PSD) is the most common neuropsychological complication of stroke, with a prevalence of ~33% (1) in stroke survivors. PSD adversely influences outcomes by reducing quality of life, increasing caregiver burden, and increasing early mortality as much as ten-fold (2–4). As acute stroke interventions continue to improve, stroke survivorship and associated morbidity will also increase, making the need to explore innovative treatments for PSD even more urgent.
Despite the significant clinical burden of PSD, there are limited treatment options to prevent or reduce its severity. Psychotherapy and pharmacotherapy are well-established as treatments of choice in major depression, however a subset of patients do not respond to either of these first-line therapies (5). Selective Serotonin Reuptake Inhibitor (SSRI) use has been associated with increased risk of hemorrhagic complications as well as increased risk of falls in the elderly, while other studies have shown that SSRIs are actually associated with increased risk for stroke, myocardial infarction, and all-cause mortality (6). A recent meta-analysis for stroke patients concluded that antidepressants did not significantly improve patients’ general recovery, achieved varied response rates, and were not tolerated due to adverse effects (7). Compliance, communication problems, and lack of access to psychiatric care are further challenges to treating PSD.
Repetitive transcranial magnetic stimulation (rTMS) may represent an effective treatment option that mitigates the issues associated with the standard PSD interventions. The FDA approved rTMS for patients with Major Depressive Disorder (MDD) in 2008 (8). The typical rTMS protocol that has been used effectively for major depression is 5 days per week for 4–6 weeks. Conventional rTMS paradigms have been studied in the PSD population, and many studies including a meta-analysis have shown that conventional rTMS is likely effective for chronic, refractory PSD (9, 10). However, these conventional paradigms may be inconvenient for patients with limited transportation access and may limit compliancy of patients. Therefore, an accelerated protocol which minimizes the number of days needed to complete the full treatment may be more accessible to patients and may increase compliancy. While there have been some accelerated rTMS paradigms that have been designed to treat conditions such as alcohol withdrawal and treatment-resistant depression (11–14), similar accelerated protocols have not been studied in patients suffering from PSD. Applying accelerated rTMS to the PSD population comes with unique and complex factors. For example, the theoretical risk of seizure using an accelerated protocol may be higher, and this risk may increase even further in patients in the acute to subacute stroke period. Therefore, it is important to study the safety of an accelerated protocol in this population. In addition, the period immediately following cerebrovascular ischemia potentially represents a biologically unique phase amenable to intervention given that both neuroplasticity as well as recurrent stroke risk are highest during this time (15, 16).
There is a clear medical need to further address the impact of rTMS for PSD and to optimize stimulation parameters. We hypothesized that an accelerated 4-days rTMS protocol would be a safe and viable method for treating PSD and would help ameliorate depressive symptoms.[…]

