Archive for October, 2020
[WEB PAGE] Durham Reading & Exploration Training – Durham University
Posted by Kostas Pantremenos in Hemianopsia on October 31, 2020

Homonymous visual field defects, such as hemianopia, involve partial blindness in both eyes which occurs following damage to the parts of the brain responsible for processing visual information. They are one of the most common and disabling consequences of brain damage, with the visual loss impacting on numerous everyday activities like crossing the street, avoiding obstacles, shopping, reading and driving.
Here in the psychology department at Durham University we have been investigating homonymous visual field defects and have been developing training programs that may be used in the rehabilitation of such impairments. The aim of our training is not to try and restore the lost vision but rather to help people to learn compensatory strategies to help them overcome the difficulties which they experience due to the visual deficit.
Our most recent training program (Durham Reading and Exploration training; DREX) is computer-based and self-adjusting, allowing people to train themselves easily in their own home. It involves a series of tasks which encourage visual exploration. These gradually get more difficult thereby promoting the development of more efficient eye-movements and increased visual awareness. Half of the training is also specifically tailored towards improving reading, a common problem associated with visual field loss. For more information about the training then please view the training details page. Please do not hesitate to get in touch with us for further information. Our details can be found on the contact us page.
Check out our blog for up to date news on our current research and events:- drexdurham.wordpress.com
[WEB PAGE] Can retraining the eyes combat hemianopia?
Posted by Kostas Pantremenos in Hemianopsia on October 31, 2020
A new study will assess the affect of providing eye scanning training to stroke survivors.
30 October 2020 by Selina Powell
 PIXABAY/LAURA ARTAL
PIXABAY/LAURA ARTAL
New research will investigate the effectiveness of eye scanning training in improving the vision and everyday independence of stroke survivors.
The collaboration between Fight for Sight and the Stroke Association was announced on World Stroke Day (October 29).
A group of 71 stroke survivors that receive eye scanning training will be compared to a control group that does not receive the training.
The study participants will be monitored for six months with information collected during routine eye clinic visits.
Eye scanning training encourages stroke survivors to look into the ‘blind’ side of their visual field, which can improve their adaptation to loss of vision.
The study will be carried out by University of Liverpool researchers and incorporate a paper-based visual scanning programme, with participants able to practise at home.
Professor Fiona Rowe, from the University of Liverpool, highlighted that the research builds on a promising pilot trial.
“Visual scanning training has the potential to benefit stroke survivors by improving their adaptation to hemianopia and it can be done at anytime, anywhere. There is also potential for cost-savings in the NHS and social care sector through maximising stroke survivors’ use of their remaining vision, and therefore lessening its impact on daily life activities,” she emphasised.
You must be logged in to join the discussion. Log in
[Abstract + References] Home-Based Rehabilitation System for Stroke Survivors: A Clinical Evaluation
Posted by Kostas Pantremenos in Paretic Hand, REHABILITATION, Spasticity, Tele/Home Rehabilitation on October 30, 2020
Abstract
Recently, a home-based rehabilitation system for stroke survivors (Baptista et al. Comput. Meth. Prog. Biomed. 176:111–120 2019), composed of two linked applications (one for the therapist and another one for the patient), has been introduced. The proposed system has been previously tested on healthy subjects. However, for a fair evaluation, it is necessary to carry out a clinical study considering stroke survivors. This work aims at evaluating the home-based rehabilitation system on 10 chronic post-stroke spastic patients. For this purpose, each patient carries out two exercises implying the motion of the spastic upper limb using the home-based rehabilitation system. The impact of the color-based 3D skeletal feedback, guiding the patients during the training, is studied. The Time Variable Replacement (TVR)-based average distance, as well as the average postural angle used in Baptista et al. (Comput. Meth. Prog. Biomed. 176:111–120 2019), are reported to compare the movement and the posture of the patient with and without showing the feedback proposals, respectively. Furthermore, three different questionnaires, specifically designed for this study, are used to evaluate the user experience of the therapist and the patients. Overall, the reported results suggest the relevance of the proposed system for home-based rehabilitation of stroke survivors.
References
- 1.Baptista R., Ghorbel E., Shabayek A.E.R., Moissenet F., Aouada D., Douchet A., André M., Pager J., Bouilland S.: Home self-training: Visual feedback for assisting physical activity for stroke survivors. Comput. Meth. Prog. Biomed. 176: 111–120, 2019Google Scholar
- 2.Emmett E., Stevens E., Cang Y., McKevitt C., Wolfe C.D.A. (2017) The burden of stroke in europe report. King’s College London for the Stroke Alliance for Europe (SAFE):2017
- 3.Veerbeek J. M., Van Wegen E., Van Peppen R., Van der Wees P.J., Hendriks E., Rietberg M., Kwakkel G (2014) What is the evidence for physical therapy poststroke? a systematic review and meta-analysis. PloS One
- 4.Langhorne P., Taylor G., Murray G., Dennis M., Anderson C., Bautz-Holter E., Dey P., Indredavik B., Mayo N., Power M., et al. (2005) Early supported discharge services for stroke patients: A meta-analysis of individual patients’ data, The Lancet
- 5.Natta D. D. N., Alagnide E., Kpadonou G.T., Stoquart G.G., Detrembleur C., Lejeune T.M.: Feasibility of a self-rehabilitation program for the upper limb for stroke patients in benin. Ann. Phys. Rehab. Med. 58: 322–325, 2015Google Scholar
- 6.Bonnyaud C., Gallien P., Decavel P., Marque P., Aymard C., Pellas F., Isner M.-E., Boyer F.C., Muller F., Daviet J.-C., Dehail P., Perrouin-Verbe B., Bayle N., Coudeyre E., Perennou D., Laffont I., Ropers J., Domingo-Saidji N.-Y., Bensmail D., Roche N. (2018) Effects of a 6-month self-rehabilitation programme in addition to botulinum toxin injections and conventional physiotherapy on limitations of patients with spastic hemiparesis following stroke (adju-tox): protocol study for a randomised controlled, investigator blinded study. BMJ Open 8
- 7.Simmons S., McCrindle R., Sperrin M., Smith A.: Prescription software for recovery and rehabilitation using microsoft kinect.. In: Pervasive Computing Technologies for Healthcare (PervasiveHealth), 2013 7th International Conference on, IEEE, 2013, pp 323–326
- 8.Spyridonis F., Gawronski J., Ghinea G., Frank A.O.: An interactive 3-d application for pain management: Results from a pilot study in spinal cord injury rehabilitation. Comput. Meth. Programs. Biomed. 108: 356–366, 2012Google Scholar
- 9.Zannatha J.M.I., Tamayo A.J.M., Sánchez A.D.G., Delgado J.E.L., Cheu L.E.R., Arévalo W.A.S.: Development of a system based on 3d vision, interactive virtual environments, ergonometric signals and a humanoid for stroke rehabilitation. Comput. Meth. Prog. Biomed. 112 : 239–249, 2013. SI: Computer Assisted Tools for Medical RoboticsGoogle Scholar
- 10.Spasojević S., Ilić N.V., Rodić A., Santos-Victor J.: Kinect-based application for progress monitoring of the stroke patients.. In: Proceedings of IcETRAN conference, vol. ROI2, Volume 6, 2017, pp 1–5
- 11.Trombetta M., Henrique P.P.B., Brum M.R., Colussi E.L., De Marchi A.C.B., Rieder R.: Motion rehab ave 3d: a vr-based exergame for post-stroke rehabilitation. Comput Meth Prog Biomed 151: 15–20, 2017Google Scholar
- 12.Antunes M., Baptista R., Demisse G., Aouada D., Ottersten B.: Visual and human-interpretable feedback for assisting physical activity.. In: European Conference on Computer Vision (ECCV) Workshop on Assistive Computer Vision and Robotics Amsterdam, 2016
- 13.Baptista R., Antunes M., Shabayek A.E.R., Aouada D., Ottersten B.: Flexible feedback system for posture monitoring and correction.. In: IEEE International Conference on Image Information Processing (ICIIP), 2017
- 14.Baptista R., Ghorbel E., Shabayek A.E.R., Aouada D., Ottersten B.: Key-skeleton based feedback tool for assisting physical activity.. In: 2018 Zooming Innovation in Consumer Technologies Conference (ZINC), IEEE, 2018, pp 175–176
- 15.Antunes M., Aouada D., Demisse G. (2017) Physical activity feedback Patent WO2017207802a1
- 16.Shabayek A., Baptista R., Papadopoulos K., Demisse G., Oyedotun O., Antunes M., Aouada D., Ottersten B., Anastassova M., Boukallel M., Panëels S., Randall G. , Andre M., Douchet A., Bouilland S., Ortiz Fernandez L. (2017) STARR – Decision SupporT and self-mAnagement system for stRoke survivoRs Vision based Rehabilitation System, European Project Space on Networks Systems and Technologies – Volume 1: EPS Porto 2017
- 17.Ghorbel E., Boutteau R., Boonaert J., Savatier X., Lecoeuche S. (2018) Kinematic spline curves: A temporal invariant descriptor for fast action recognition, Image and Vision Computing
[Abstract] Preliminary Design of a Novel Teleoperation Interface for Home-based Upper Limb Rehabilitation
Posted by Kostas Pantremenos in Paretic Hand, REHABILITATION, Rehabilitation robotics, Tele/Home Rehabilitation on October 30, 2020
Abstract
With the increasing incidence of stroke, the demand for post-stroke rehabilitation is also increased. Various rehabilitation devices have been proposed to facilitate home-based rehabilitation and reduce the therapist’s workload. This paper presnets a novel teleoperation interface to allow the therapist in the hospital to guide the patient’s rehabilitation at home via TCP/IP communication. In order to achieve safe and comfortable home-based rehabilitation, the proposed teleoperation interface implements independent position and stiffness control to remotely guide the operation of the exoskeleton device worn on the patient. The preliminary experimental results showed that the proposed tele-rehabilitation was capable of providing effective power assistance and stiffness adjustment in real time under the guidance of the therapist.
[Abstract] Design and Analysis of a Wearable Exoskeleton Upper Limb Rehabilitation Robot
Posted by Kostas Pantremenos in Paretic Hand, REHABILITATION, Rehabilitation robotics on October 30, 2020
Abstract
In order to solve the disadvantages of the large size of the braced upper limb rehabilitation robot, a wearable upper limb exoskeleton robot was designed. Firstly, a 3D model of the robot was built using SOLIDWORKS based on the principle of modularity. According to the structural characteristics of the wearable upper exoskeleton robot, choose the driving mode of the robot and the installation position of the motor reasonably. Secondly, the kinematic analysis of the robot was performed using the D-H parameter method. Finally, the model was imported into ADAMS for motion simulation of shoulder joint flexion/extension, adduction/abduction and elbow joint flexion/extension. Simulation results prove that the rehabilitation robot has a well-designed shoulder and elbow joint structure, smooth motion curve, no sudden changes in speed and position, and good bionic properties. The conclusion is the wearable upper limb rehabilitation robot is well designed, can provide patients with effective rehabilitation training. A theoretical basis for future prototype production and subsequent research was laid.
[Abstract] Attention Enhancement and Motion Assistance for Virtual Reality-Mediated Upper-limb Rehabilitation
Posted by Kostas Pantremenos in Paretic Hand, REHABILITATION, Video Games/Exergames, Virtual reality rehabilitation on October 30, 2020
Abstract
Dysfunctions of upper limbs caused by diseases such as stroke result in difficulties in conducting day-to-day activities. Studies show that rehabilitation training using virtual reality games is helpful for patients to restore arm functions. It has been found that ensuring active patient participation and effort devoting in the process is very important to obtain better training results. This paper introduces a method to help patients increase their engagement and provide motion assistance in virtual reali-ty-mediated upper-limb rehabilitation training. Attention en-hancement and motion assistance is achieved through an illusion of virtual forces created by altering the drag speed between the cursor and the object presented on a screen to the patient as the only feedback. We present two game forms using the proposed method, including a target-approaching game and a maze-following game. The results of evaluation experiments with human participants showed that the proposed method could provide path guidance that significantly improved path-following performance of users and required more involvement of the users when compared to playing the game without attention enhance-ment and motion assistance.
[ARTICLE] Prediction of Motor Recovery in the Upper Extremity for Repetitive Transcranial Magnetic Stimulation and Occupational Therapy Goal Setting in Patients With Chronic Stroke: A Retrospective Analysis of Prospectively Collected Data – Full Text
Posted by Kostas Pantremenos in Paretic Hand, REHABILITATION, tDCS/rTMS on October 30, 2020
Recovery from motor paralysis is facilitated by affected patients’ recognition of the need for and practice of their own exercise goals. Neurorehabilitation has been proposed and used for the treatment of motor paralysis in stroke, and its effect has been verified. If an expected score for the neurorehabilitation effect can be calculated using the Fugl-Meyer Motor Assessment (FMA), a global assessment index, before neurorehabilitation, such a score will be useful for optimizing the treatment application criteria and for setting a goal to enhance the treatment effect. Therefore, this study verified whether the responsiveness to a treatment method, the NovEl intervention using repetitive transcranial magnetic stimulation and occupational therapy (NEURO), in patients with post-stroke upper extremity (UE) motor paralysis could be predicted by the pretreatment FMA score. No control group was established in this study for NEURO treatment. To analyze the recovery of the motor function in the UE, delta-FMA was calculated from the pre- and post-FMA scores obtained during NEURO treatment. The probability of three levels of treatment responsiveness was evaluated in association with delta-FMA score (<5, 5 ≤ delta-FMA <10, and ≥10 as non-responders; responders; and hyper-responders, respectively) according to the reported minimal clinically important difference (MCID). The association of the initial FMA scores with post-FMA scores, from the status of the treatment responsiveness, was determined by multinomial logistic regression analysis. Finally, 1,254 patients with stroke, stratified by FMA scores were analyzed. About 45% of the patients who had FMA scores ranging from 30 to 40 before treatment showed improvement over the MCID by NEURO treatment (odds ratio = 0.93, 95% CI = 0.92–0.95). Furthermore, more than 25% of the patients with more severe initial values, ranging from 26 to 30, improved beyond the MCID calculated in the acute phase (odds ratio = 0.87, 95% CI = 0.85–0.89). These results suggest that the evaluated motor function score of the UE before NEURO treatment can be used to estimate the possibility of a patient recovering beyond MCID in the chronic phase. This study provided clinical data to estimate the effect of NEURO treatment by the pretreatment FMA-UE score.
Introduction
Motor paralysis due to the aftereffects of stroke impairs the activities of daily living (ADL) and quality of life (QOL) of patients; it also affects their individual or social activities (1, 2). In particular, motor paralysis of the upper extremity has a large impact on ADL (3). Recovery from motor paralysis is facilitated by patients recognizing the need for and practicing their own exercise goals (4). The type of goals that patients set are related to their goal satisfaction scores, with impairment-based goals being rated significantly higher than activity-based and participation-based goals (5). It is known that patients’ level of knowledge of their rehabilitation goals leads to effective treatment results (6). Thus, clinicians and patients are active partners in setting goals within stroke rehabilitation (5). In previous studies, some prognosis prediction systems were developed for motor paralysis (7–9), and they have been used to set goals for rehabilitation in patients with stroke.
Neurorehabilitation has been proposed and used for the treatment of motor paralysis in stroke, and its effect has been verified (10–14). One of the treatment methods, the NovEl intervention Using Repetitive transcranial magnetic stimulation and Occupational therapy (NEURO), facilitates peripheral muscle movement by controlling the excitability of the motor cortices by repetitive transcranial magnetic stimulation (rTMS). It also promotes peripheral muscle exercise and practice, for the active use of the paralyzed upper extremity (15, 16). NEURO’s efficacy has been proved in a randomized controlled study (17). To date, many patients have been treated by using NEURO; however, the prediction regarding whether patients’ recovery from motor paralysis after treatments can be predicted before treatment, has not been verified. If the Fugl-Meyer Motor Assessment (FMA) score before treatment can be used to predict NEURO treatment response, the score can be used as an effective goal for rehabilitation, by patients and therapists.
The minimal clinically important difference (MCID) of motor paralysis in the upper extremity has been investigated (18–20). If the expected value of an effect exceeding MCID can be calculated using FMA score measured before NEURO treatment, such a value will be useful for optimizing the treatment application criteria and setting a goal to enhance the treatment effect. For that purpose, it is sufficient to retroactively analyze the band of the FMA score before NEURO for a patient who is significantly improved. Therefore, this study verified whether the responsiveness of NEURO treatment for patients with post-stroke upper extremity motor paralysis could be predicted by the pre-treatment FMA score.[…]
[QUOTATION] Caregivers go through…
Posted by Kostas Pantremenos in Caregivers, Quotations on October 29, 2020

[ARTICLE] F@ce: a team-based, person-centred intervention for rehabilitation after stroke supported by information and communication technology – a feasibility study – Full Text
Posted by Kostas Pantremenos in REHABILITATION, Tele/Home Rehabilitation on October 27, 2020
Abstract
Background
Globally, there is a growing use of Information and Communication Technology (ICT), including mobile phones, tablets and computers, which are being integrated into people’s daily activities. An ICT-based intervention called F@ce was developed in order to provide a structure for the process in stroke rehabilitation and facilitate change by integrating a global problem-solving strategy using SMS alerts. The aim of the study was to evaluate the feasibility of i) F@ce within in-patient and primary care rehabilitation after stroke, ii) the study design and outcome measures used, and iii) the fidelity, adherence and acceptability of the intervention.
Methods
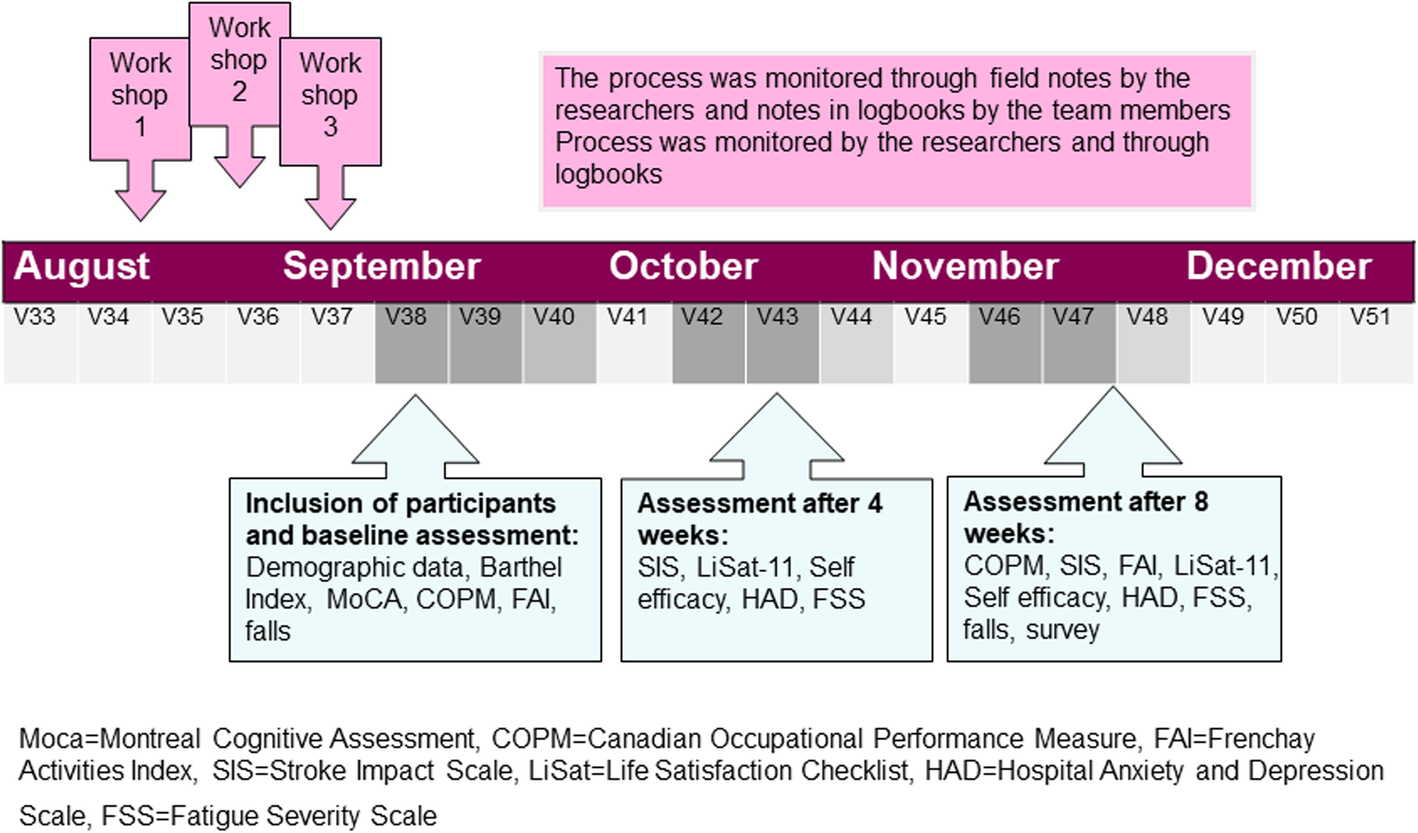
Three teams comprising occupational therapists and physiotherapists who work in neurological rehabilitation participated in a preparatory workshop on F@ce and then enrolled 10 persons with stroke to participate in the intervention. Goals were set using the Canadian Occupational Performance Measure (COPM) and the participants with stroke rated their performance and satisfaction with the activities associated with the three goals every day for 8 weeks. Data were collected at inclusion, at four and 8 weeks, using the COPM, Stroke Impact Scale, Frenchay Activities Index, Life Satisfaction Checklist, Self-Efficacy Scale, Hospital Anxiety and Depression Scale, Fatigue Severity Scale, follow-up survey, daily ratings on the web platform and logbooks.
Results
All of the participants showed increased scores in the primary outcome (COPM) and a clinically meaningful improvement of ≥2 points was found in four participants regarding performance and in six participants regarding satisfaction. Overall fidelity to the components of F@ce was good. The response rates to the F@ce web platform were 44–100% (mean 78%). All of the participants stated that F@ce had supported their rehabilitation.
Conclusion
The results indicate that the most beneficial part of F@ce was the person-centred, goal-setting process and SMS alerts. All participants were satisfied with F@ce and highlighted the benefits of receiving daily alerts about their goals. This encouraged them to be more active. The only downside mentioned was that they felt under an obligation to practice, although this was described as “a positive obligation”.
Background
Digitalisation in society, as well as in health care and rehabilitation, has increased rapidly in recent years [1, 2]. In line with this development, the Swedish government has created a vision of becoming a global leader in digital health solutions by 2025 [2]. Digitalisation can be a valuable tool for increased participation in society for people with disabilities as after stroke [3, 4]. There are a range of concepts and definitions that address different aspects of digitalisation in health care such as e-health, tele rehabilitation and health informatics. In this study, the term Information and Communication Technology (ICT) is used, including all technologies that are used interactively for communication and transfer of information, such as mobile phones, tablets and computers, as well as the applications and software of such devices [5].
The ability to manage activities in daily living (ADL) and participate in everyday life, including work, leisure and social activities, is often restricted after a stroke [6,7,8,9]. Thus, the everyday life after stroke has been described as chaotic and receiving rehabilitation to manage ADL is often a priority [8, 10]. The development of more user-friendly ICT solutions has created opportunities to provide ICT-supported rehabilitation services that could reduce some of the unmet needs of rehabilitation that are reported by people who have had stroke [9]. Although the evidence concerning the effectiveness of ICT is inconclusive [3, 4], a recent review has shown that interventions using ICT have beneficial effects on motor, higher cortical and mood disorders [4]. It has also been shown that ICT used as an alternative to face-to-face interventions could improve participation in daily life after stroke [3].
ICT could be utilised in rehabilitation after stroke to monitor rehabilitation progress and interact at a distance [3, 4]. The use of a mobile phone or computer has been shown to promote participation in everyday life and create a sense of security [11, 12]. Furthermore, the use of ICT-based interventions could reduce the number of home visits, thereby saving time and travel costs, particularly in rural areas [12, 13]. ICT solutions have also shown to enable person-centred care [14, 15] and facilitate communication and feedback from healthcare professionals [3, 16]. A concern among people with stroke is their potentially limited ability to manage different ICT devices. Earlier research has found that people could encounter a range of difficulties [11, 17, 18] but that people with acquired brain injury such as stroke could benefit from using ICT in their daily lives [11, 19]. Moreover, ICT could be successfully introduced and used within rehabilitation after acquired brain injury, regardless of age or previous use [20]. However, support is often needed, particularly when using a new device or when something unexpected happens [11].
A client-centred ADL intervention (CADL) was developed with the aim of enabling agency in activities and participation in everyday life among persons with stroke [21, 22]. The CADL was based on phenomenology with the lived experiences of the person as a point of departure for the intervention [23]. The client-centred approach included building a therapeutic relationship and ensuring that the person was actively involved in the goal setting and planning of the rehabilitation [24,25,26]. The CADL was delivered by occupational therapists and evaluated in a randomized controlled trial (RCT) [21, 22] along with qualitative studies [27,28,29]. The results of the RCT [21, 22] were inconclusive but the qualitative studies emphasized that sharing [28] and transparency [29] between therapists and the patients were benefits of using a client-centred approach. It was also shown that the CADL appeared to enhance the involvement of patients in goal setting and individualisation of the rehabilitation. In the present study, the CADL was further developed by following the Medical Research Council (MRC) guidelines for the development of complex interventions [30].
The results of the CADL study is a part of the evidence base in the development of the new intervention called F@ce that is presented in this study. One conclusion from the CADL evaluations was that all members of a stroke rehabilitation team should use the intervention. This is also recommended in the Swedish national guidelines for stroke care [31] and in this new intervention F@ce, the multidisciplinary teams were included. In line with the new multidisciplinary approach, the term client-centred was replaced with person-centred. The terms client-centred and person-centred are based on the same underlying theories as described by Rogers [32]. The person-centred approach views the person as having the potential to change and the therapist as being a facilitator in this process [32, 33].
The potential benefits and obstacles for using ICT within a person-centred rehabilitation intervention for people after stroke remain largely unexplored. Although healthcare professionals and persons with stroke have reported high levels of acceptance and satisfaction when using ICT interventions in stroke care, few studies have explored the outcome of such interventions [3, 34]. Thus, to meet the vision of the Swedish government [2], further research on the development and use of ICT within rehabilitation is needed.
Our assumption was that ICT could be used as a tool for reinforcing person-centred rehabilitation through increased sharing [28] and transparency [29]. According to the MRC guidelines, an important stage in the development of new interventions is conducting a feasibility study before testing on a larger scale [30]. Thus, this study had the following aim: to evaluate the feasibility of i) F@ce within in-patient and primary care rehabilitation after stroke, ii) the study design and outcome measures used, and iii) the fidelity, adherence and acceptability of the intervention.[…]
[ARTICLE] Multi-Sensor Validation Approach of an End-Effector-Based Robot for the Rehabilitation of the Upper and Lower Limb – Full Text
Posted by Kostas Pantremenos in Paretic Hand, Rehabilitation robotics on October 27, 2020
Abstract
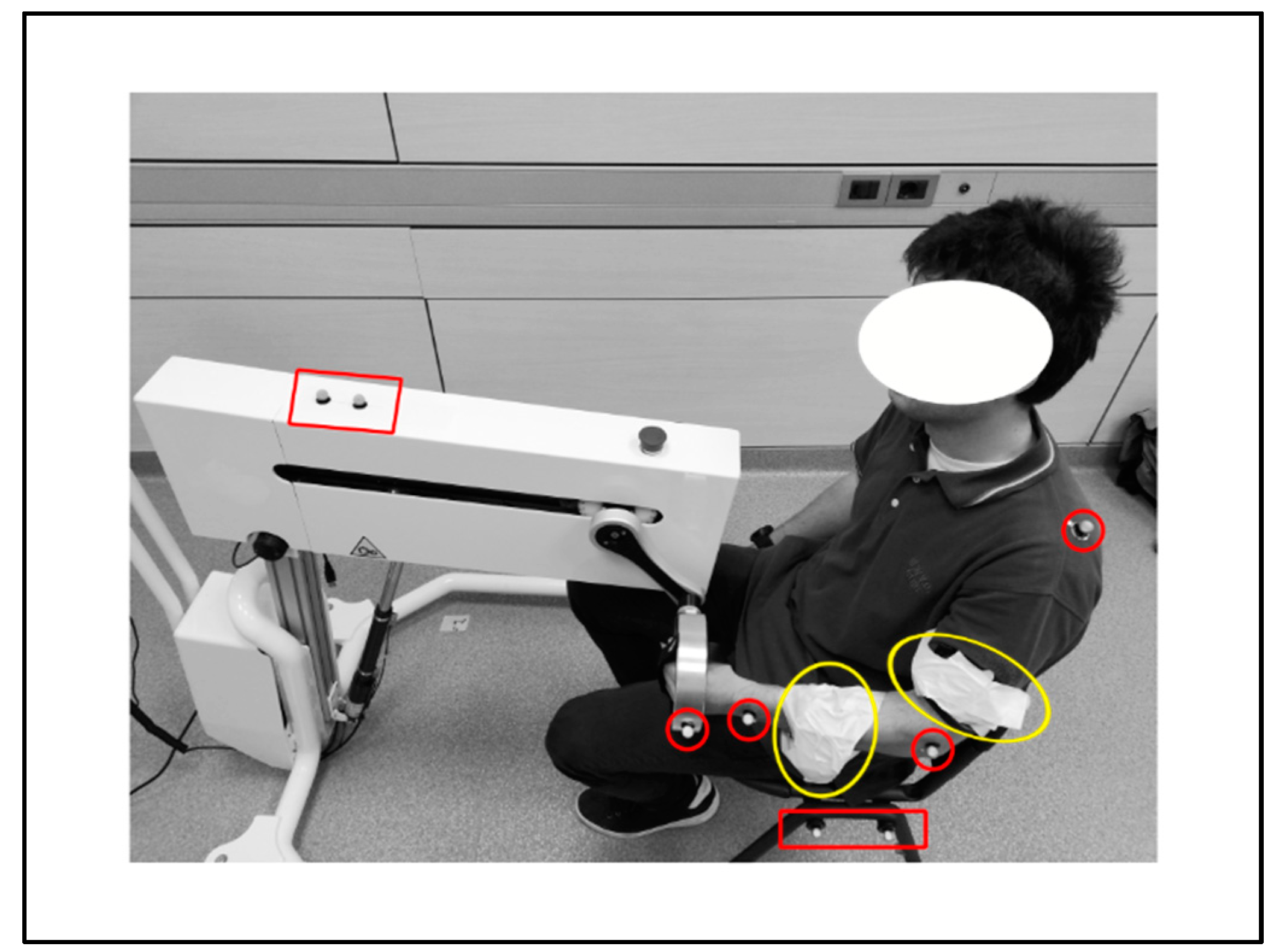
End-effector-based robots are widely adopted by physiotherapists and caregivers as support in the delivery of the rehabilitation training to the patient. The validation of these devices presents critical aspects, since the system performance must be assessed analyzing the movement performed by the subject limb, i.e., elements outside the device. This paper presents a multi-sensor approach for the validation of an innovative end-effector-based device, comparing different measurement strategies for evaluating the system effectiveness in imposing an expected training. The study was performed monitoring the movement induced by the device on the upper limb of a young male healthy subject during a set of fictitious rehabilitation sessions. The kinematic structure of the device is characterized by a compact differential mechanism with two degrees of freedom. A sequence of repetitions of a planar reaching pattern was analyzed as illustrative training task. A kinematic model of subject and system was developed, and the kinematics of a set of specific landmark points on the subject limb was evaluated. Data obtained from two measurement systems were compared: (1) an optoelectronic system with two cameras and eight skin passive markers, and (2) two triaxial accelerometers. Results were analyzed in MATLAB and R environment, revealing a high repeatability of the limb movement. Although both the measurement systems allow evaluating the acceleration of subject’s arm and forearm, accelerometers should be preferred for punctual analysis, like components optimizations, whereas optical markers provide a general overview of the system, particularly suitable for the functional design process.
1. Introduction
The motor skills reduction in subjects affected by neurologically based disorders, like stroke, spinal cord injuries and traumatic brain lesions, strongly influences the quality of life [1,2,3]. In particular, the ability of independently and self-sufficiently execute everyday motor tasks is greatly reduced by extremities functional limitations [4]. For this reason, more than restoring the capacity of realizing a task in the natural way, the primary aim of rehabilitation techniques is allowing the execution of the lost motor functions, re-educating the subjects to coordinate movements. Besides, motor and neuro-motor rehabilitation, combined with the use of orthoses and functional electrical stimulation, improves also the subject mental abilities and prevents secondary complications such as spasticity, muscle atrophy and osteoporosis [5].The physical rehabilitation process begins with a preliminary analysis of the patient’s residual abilities, suitable for identifying the most effective rehabilitation protocol. According to literature, biofeedback and robot-assisted therapy, as well as virtual reality training, intensify the rehabilitation therapy allowing the accurate repetition of motor patterns [6]. Indeed, onset, intensity, duration and task-orientation of the training significantly affect the achievement of positive outcomes. As literature enlightens, repetitive training generates functional improvements which depend on patients inclusion criteria and time elapsed from the stroke, but also on the repetitions quantity [7]. In fact, scientific evidences suggest to extend the duration of training sessions, since longer sessions have better effects on motor functions [7,8].In recent literature, many works deal with the use of robotic devices for rehabilitation purposes, offering a wide variety of solutions for the upper and lower limbs rehabilitation, both in clinical environments and at home [5,9,10,11]. Several devices may provide a different kind of motion assistance, like passive or active mobilization, as well as haptic assistance or coaching [9]. Active devices, presenting at least one actuator, can induce the movement of specific parts of the limb, performing active or passive exercises. Moreover, the device may support the subject, which actively performs the task by moving the limb; on the contrary, in passive exercises the patient movement is guided by the device during the rehabilitation session.An alternative taxonomy classifies devices considering the mechanical design. Actually they can be (1) end-effector-based, i.e., the contact between machine and patient’s limb arises only at the end-effector level (e.g., MIT Manus [12]), or (2) exoskeleton-based, in which the mechanical configuration of the device mirrors the limb’s skeletal structure [13,14,15]; in those devices the contact between subject and system is distributed along the limb with multiple contact areas. Literature also presents many devices that combine these two structures, like the MIME-RiceWrist rehabilitation system [16].Besides, some devices are characterized by specific and significant features. Among them, reconfigurability represents the capability of the system of changing its mechanical structure, adapting it to different use conditions, or the ability to follow the subject necessities (e.g., MUNDUS [6]). Back-drivability describes instead the possibility of the patient to induce the movement of the system when the device is in passive state (e.g., HWARD [17]). Mechanical structure of the system, as well as type, number and location of the actuators determine the allowed movements of the device and the degrees of freedom (DOFs) of the system consequently. As the literature reports, most of the devices allow three-dimensional movements [18], whereas only a restricted group of devices enable the movement on a specific plane (e.g., ARC-MIME [19]).Focusing on the control of the devices, several signals may be evaluated, like externally imposed triggers [20], kinematic or dynamic signals from the device [21,22], as well as biomechanical signals from the subject, such as data derived from surface electromyography (sEMG [23,24]). Nonetheless, biomechanical systems can be considered characterized by low dynamics phenomena, and rehabilitation training even more, given the low velocities required for a correct training [25].Literature provides numerous examples of multi-sensor validation in clinical or rehabilitative contexts when considering the human motion [26,27], whereas multiple units of the same sensor are generally used when validating devices [28].Within this complex context, the validation process of new rehabilitation devices becomes critical, since the true analysis dimension for evaluating the system performance coincides with the analysis of the motion performed by the subject, referring therefore to elements outside the device. Hence, the system to monitor can include the device, but mainly focuses on the final user, i.e., the patient. We can describe some validation methods as device-oriented, meaning that the validation is pursued through the comparison of the performance, as recorded by the rehabilitation system, with those detected by the sensors located along the device. This is the typical condition for exoskeleton devices, in which the design of the system, with the distributed contact between machine and subject, justifies the hypothesis of negligible approximation errors between motion profile realized by device and movement of the patient limb. In this case, sensors like the inertial measurement unit (IMU) [29] or camera-based systems [30] are mostly used. Besides, according to the same rationale, other validation methods can be defined as user-oriented, since the analysis is performed detecting the patient movement, thanks to wearable sensors like EMG sensors [31] and optoelectronic systems [29] placed on significant landmarks of the testing subjects. This approach is necessary for end-effector based devices, since the process to monitor is partially independent from the device constraints, and differently from the device-oriented methods, it demands for the identification of a proper kinematic or dynamic model of the subject.In this work a multi-sensor validation approach is investigated and an innovative rehabilitation device was considered for the study. The device is an end-effector-based robotic system that has been developed within the SIMeRiON (Innovative Mechatronics System for Orthopedic and Neurological Rehabilitation) project, funded by Regione Lombardia [32]. The device is back-drivable and reconfigurable, presents an electro-mechanical actuation system, and is able to provide passive, active and assisted rehabilitation [32,33]. The mechanical system is based on a compact differential system and is characterized by two DOFs; this allows implementing every kind of motion profile within a plane. The device performance is analyzed evaluating the movement induced by the device on the upper limb of a healthy subject in a sequence of repetitions. The movement characteristics are investigated monitoring specific landmark points of the subject’s limb, with the aim of verifying the system effectiveness in imposing the expected training. The kinematics of those points has been detected thanks to (1) an optical marker-based tracking system, and (2) an inertial sensor-based system. Acquired data have been compared to evaluate strength points and drawbacks of each measuring strategy for the proper tuning of the system model; in fact, the kinematic model of subject and system has been defined and used as reference for the interpretation of the collected data. In the next section, a synthetic description of the device is reported, and the adopted methods for the performed data treatment are described. Results are then presented and discussed in the following sections, whereas main strength points and limits of the work are finally described in the conclusions.[…]
-
You are currently browsing the archives for October, 2020

