This study investigated the effects of cognitive exercise therapy on upper extremity sensorimotor function and daily activity in patients with chronic stroke and compared these effects to those of conventional occupational therapy. The 30 patients with chronic stroke (mean age: 63.6 ± 12.7 years; height: 162.8 ± 8.1 cm; weight: 60.6 ± 7.6 kg; body mass index: 22.8 ± 1.9 kg/m2) were divided into two treatment groups with 15 patients in each. The respective interventions were provided for 30 min per day, five times weekly for 4 weeks. Manual and sensory function tests were conducted to evaluate the sensorimotor function, while the Korean-Modified Barthel Index was used to assess daily activities. All outcome variables were assessed before and after the interventions. A significant interaction was observed in sensory function (p = 0.001) but not motor function or daily activities (p > 0.05). No significant main group effects were found for any outcome variables (p > 0.05). The experimental group showed significant improvements in motor function (p < 0.001), sensory function (p < 0.001), and daily life activities (p = 0.001) after cognitive exercise therapy, whereas the control group showed significant improvement only in daily life activities post-intervention (p = 0.012). These results demonstrated the positive effects of cognitive exercise therapy on upper extremity sensorimotor function and daily life activities and the lack of improvement in motor and sensory function following conventional occupational therapy in patients with chronic stroke. Thus, the combination of cognitive exercise and conventional occupational therapies may be an effective way to improve sensory function and upper extremity motor function in patients with chronic stroke.
1. Introduction
A stroke, a sudden impairment of body function caused by a blockage of blood flow to the brain, has the third-highest mortality rate after cancer and heart disease [1,2]. More than 85% of patients with stroke experience hemiplegia, and 55–75% of these patients have upper extremity impairment [3]. Impaired upper extremity function may result in decreased mobility of the shoulder joint, muscle weakness, sensory impairment, spasticity, and lack of coordination [4]. Subsequently, these lead to sequelae such as limited joint movement and limited upper extremity function [5]. Sensory impairment occurs in at least 50% of stroke patients and is expected to be higher with accurate examinations [6]. Sensory impairment interferes with correct movement and sharply reduces movement based on sensory input or feedback [7]. Patients with sensory impairment avoid movement, and their movements are dull and uncoordinated [7,8]. Thus, for patients with sensory impairment, proprioception, tactile sensation, pressure sensation, and stereoscopic sensation are essential for smooth movement by activating natural movements [9]. As these sensations are closely related to functional recovery after stroke, the impaired sensory function is one of the most significant factors hindering rehabilitation in patients with stroke. Additionally, impairment of upper extremity and sensory functions reduce the performance of basic daily activities. Therefore, patients cannot perform these activities independently and rely on the help of their caregivers [10].
Many interventions have been applied to address upper extremity function in patients with stroke. Among these, task-oriented upper extremity training improved the function of affected upper extremities [11,12,13]. The complex interaction between the left and right brains during bilateral tasks of the upper extremities enhanced the function of the affected upper extremity [11,12]. Moreover, constraint-induced movement therapy in the affected upper extremity of patients with stroke improved upper extremity function [13]. However, these interventions are therapeutically accessible only to patients with at least minimal voluntary motor skills. Another intervention is mirror therapy, which reorganizes brain areas along with physical rehabilitation. Based on the theoretical mirror neuron system, this intervention method promotes functional recovery of the upper extremities by inducing the recovery of motor function and movement on the affected side [14]. Another invention is mental practice, which allows patients to acquire and improve motor skills through thoughts of certain movements rather than actual body movements [15]. When a certain level of sensory recovery can be expected, repeated stimulation may provide necessary sensory feedback; moreover, the senses may be improved to a conscious level by focusing on a given sense [16].
Cognitive exercise therapy is a therapeutic intervention that aims to reorganize the central nervous system through learning motor function recovery [17,18]. This therapy emphasizes the close relationship of motor function to the activation of cognitive processes in the brain, such as perception, attention, memory, judgment, and language. The quality of recovery depends on the correct identification of the cognitive factors [19]. Cognitive exercise therapy allows various movements or actions to be performed through cognitive training processes, rather than movement training through interaction between the body and environment, to build a brain schema with four principles. The first principle is ‘attention’, which focuses on enhancing the effectiveness of treatment and reorganizing exercises in the treatment process. Second, patient treatment requires attention to somatosensory information with the eyes closed. Third, specific treatment instruments or tools are used to treat cognitive problems through interactions between the body and the environment. Finally, cognitive exercise does not force patients to conduct muscle contractions to accurately mobilize motor units. As such, the purpose of cognitive exercise therapy is not to teach patient-specific body postures but rather to develop and maximize the ability to organize the spatial, temporal, and intensity factors of the exercise sequence in the interaction between the body and environment [20].
Studies on cognitive exercise therapy in patients with stroke have shown improved upper extremity functions such as motor function, manual skills, and strength through image training of cognitive exercise therapy [21]. A comparison of cognitive exercise profiles showed improvements in sensory recognition and movement in the paralyzed arm [22]. In another study, activities of daily living (ADL) and motor function of the upper extremity improved after cognitive exercise therapy through contact tasks using a sponge on the paralyzed arm and spatial tasks using a graphic panel in patients with acute stroke. In addition, cognitive exercise profiling improved joint angle, spatiality, and shape recognition in recognition patterns [23].
However, most studies on cognitive exercise therapy were single-case or single-group studies with non-randomized groups and without a control group. Thus, these effects have not been directly compared. In addition, while various assessments have been conducted on upper extremity functions and daily activities, changes in cognitive patterns and pathological characteristics were described rather than used to directly assess sensory function recovery, which is a key factor in cognitive exercise therapy. While this approach is suitable for a single case study or qualitative research with a small number of subjects, it is difficult to quantify the objective results. Therefore, this study evaluated the effects of cognitive exercise therapy and compared them to conventional occupational therapy on upper extremity motor function, sensory function, and daily activities in patients with chronic stroke. We hypothesized that cognitive exercise therapy would improve upper extremity motor and sensory function and daily activities compared to conventional occupational therapy.[…]
Figure 2 (A) Shoulder joint recognition training by motor imagery. (B) Shoulder and elbow joint recognition training using a circular track plate. (C) Training on awareness of elbow and wrist joint angles using a Bogen. (D) Training on pressure awareness of the elbow and wrist using a sponge. (E) Finger tactile recognition training using a tactile plate.
In the recent years, the use of virtual reality (VR) to enhance motor skills of persons with activity and participation restriction due to disease or injury has become an important area of research and translation to practice. In this chapter, we describe the design of such VR systems and their underlying principles, such as experience-dependent neuroplasticity and motor learning. Further, psychological constructs related to motivation, including salience, goal setting, and rewards are commonly utilized in VR to optimize motivation during rehabilitation activities. Hence, virtually simulated activities are considered to be ideal for [1] the delivery of specific feedback, [2] the ability to perform large volumes of training, and [3] the presentation of precisely calibrated difficulty levels, which maintain a high level of challenge throughout long training sessions. These underlying principles are contrasted with a growing body of research comparing the efficacy of VR with traditionally presented rehabilitation activities in persons with stroke that demonstrate comparable or better outcomes for VR. In addition, a small body of literature has utilized direct assays of neuroplasticity to evaluate the effects of virtual rehabilitation interventions in persons with stroke. Promising developments and findings also arise from the use of off-the-shelf video game systems for virtual rehabilitation purposes and the integration of VR with robots and brain-computer interfaces. Several challenges limiting the translation of virtual rehabilitation into routine rehabilitation practice need to be addressed but the field continues to hold promise to answer key issues faced by modern healthcare.
References
Burdea GC, Coiffet P. Virtual reality technology. Presence. 2003;12(6):663–4.
Slater M. Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philos Trans R Soc B Biol Sci. 2009;364(1535):3549–57.
Slater M, Wilbur S. A framework for immersive virtual environments (FIVE): Speculations on the role of presence in virtual environments. Presence. 1997;6(6):603–16.
Llorens R, et al. Tracking systems for virtual rehabilitation: objective performance vs subjective experience: a practical scenario. Sensors. 2015;15(3):6586–606.
Sensorimotor impairments of the hand after stroke can drastically reduce the ability to perform activities of daily living. Recently, there has been an increased interest in minimally supervised and unsupervised rehabilitation to increase therapy dosage and to complement conventional therapy. Several devices have been developed that are simple to use and portable. Yet, they do not incorporate diversified somatosensory feedback, which has been suggested to promote sensorimotor recovery. Here we present the prototype of a portable one-degree-of-freedom hand trainer based on a novel compliant shell mechanism. Our solution is safe, intuitive, and can be used for various hand sizes. Importantly, it also provides rich sensory feedback through haptic rendering. We complement our device with a rehabilitation game, where we leverage interactive tangible game elements with diverse haptic characteristics to provide somatosensory training and foster recovery.
For individuals with hand hemiparesis following a stroke, rehabilitation strategies are predominantly founded on the principles of neuroplasticity and automaticity [1] to regain optimal hand-related functional abilities and facilitate participation in everyday activities. Such an approach requires to engage these individuals into meaningful activity-specific exercises and to repeat those intensively on a daily basis. Adhering to these principles [2] remains challenging in clinical practice for rehabilitation professionals, especially given various time and productivity constraints. To overcome this challenge, the development of soft robotic gloves to facilitate hand rehabilitation have progressed substantially in the last decade. Moreover, these soft robotic gloves are foreseen as promising rehabilitation intervention to potentiate the effects of conventional rehabilitation interventions and are now about to transition into clinical practice, although their effects remain uncertain given the paucity of evidence. In this context, this review aims to map evidence on the effects of the different rehabilitation interventions using a soft robotic device for sensorimotor hand impairments and, whenever possible, the satisfaction related to their use.
METHODS
Eligibility Criteria, Information Sources, And Search
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [3]. A review of the literature published in English and French from 2000 to October 2018 using a combination of search terms was conducted in Medline, EMBASE, and CINAHL. The search strategy included a combination of search terms related to three key domains: technology attributes (robotics, bionics, exoskeleton device, robot*, exoskelet*, motorized, motor-driven, motor assisted), anatomy of the hand (hand, hands, wrist*, finger*, prehension, dexterity), and rehabilitation domains (rehabilitation, exercise*, exercise therapy, physical therapy modalities, physical therapy speciality, physical therapists, occupational therapy, occupational therapist, therap*, physiothrap*). Search terms related to amputation, surgery, computer-assisted device, and teleoperation were excluded. From this initial search, 1870 articles were found and only 1206 articles remained after eliminating all duplicates. To narrow down the number of articles, a new domain was added (i.e., technology= glove, soft, wearable) and the search among the keywords, title, and abstracts was continued in EndNote. Thereafter, 181 articles remained and were imported into the web-based software platform Covidence where 9 additional duplicates were found.
SELECTION OF SOURCES OF EVIDENCE
The articles title, abstract and full text of 172 articles were screened by two rehabilitation professionals to identify the articles qualifying for a subsequent full review. To be considered for full review the article has to target 1) the effects or effectiveness of rehabilitation interventions using soft robotic gloves to optimize hand-related functional abilities and facilitate participation in everyday activities in people with sensorimotor disorders via randomized controlled trials (RCTs), non-randomized controlled trials (non-RCT), and other types of research designs (cohort studies, pre- and post-case interventions, case series, case-control studies and case reports) and 2) the users satisfaction and stakeholder views on the use of soft robotic gloves. For this review, in order to be considered a soft robotic glove, the technology had to generate assisted pinching or gripping movements soliciting multiple joints involving at least the thumb and the index finger and middle fingers. Interventions using a soft robotic glove could be performed in a hospital, rehabilitation center or at home with the direct or indirect supervision of a rehabilitation professional. The use of the soft robotic glove could also be combined with other technologies (e.g., virtual reality). Research protocols or manuscripts that did not include participants with sensorimotor impairment were excluded. All scientific manuscripts and conference abstracts focusing on upper limb exoskeleton including the elbow or shoulder joint were excluded.
Data Extraction And Charting Process
Studies that met the inclusion and exclusion criteria were read by a single rehabilitation professional and the following information were extracted on project-specific forms data extraction tables organized within an excel file: author-related information’s, journals and publication year, soft robotic glove attributes, study design, population and sample size, intervention, measurement instruments, results and interpretations, and user’s satisfaction. At the end, to establish if the use of a soft robotic glove yield to positive, neutral or negative effect, the p-value and effect size of each outcome measures from each article were determined.
RESULTS
Characteristics Of Sources Of Evidence
Ten articles included in this study originated from European or American countries; USA (5/10) [4-8], Italy (2/10) [9,10], United Kingdom (2/10) [11,12], and Netherlands (1/10) [13]. The majority of these studies were published in 2017 (6/10) [6,8-12] or 2018 (3/10) [5,7,13]. Only one study was published in 2011 [4].
Study Designs And Populations
Both experimental (3/10) [8,10,12] and quasi-experimental studies (7/10) [4-7,9,11,13] were selected with mean sample sizes of 12,4 participants and ranging from 2 to 27. Most studies investigated individuals with hemiparesis following a stroke (9/10) [4-6,8-13] whereas one article investigated individuals with of a traumatic spinal cord injury [7].
Synthesis Of Findings
Soft robotic gloves
Eight different soft robotic gloves (i.e., HandSOME [4,6], FES Hand Glove [7], Gloreha Light Glove [9], Gloreha Professional [10], VAEDA [8], HandinMind [12,13] and two others without names) with different types of assistance (i.e., motor [7,8,9,10,12,13], elastic [4,6], and pneumatic [5,11]) were identified.
Interventions
Four studies [4,5,11,13] used a transversal design to compare hand function with and without the use of a soft robotic device glove whereas three studies used an experimental design [8,10,12] and three used a quasi-experimental design [6,7,9] to compare hand sensorimotor integrity and functional abilities before and after an intervention with the soft robotic glove. No concomitant therapy was used in all of the studies. The intervention protocols of the experimental and quasi-experimental design studies varied in length from 4 to 8 weeks, in frequency from 3 to 6 times a week and training sessions duration from 40 to 90 minutes.
Outcome measures
The outcome measures included: Ashworth Spasticity Index [9] or Ashworth modified scale [6], edema [9], Hand pain VAS [9], Barthel [9], Motricity index [9,10], Nine hole peg test (NHPT) [9,10], grip strength [4,6,8-10], active range of motion (AROM) [4], Velocity of movements [4], Box and blocks test [4], Fugl-Meyer Assessment of Upper Extremity (FMA-UE) [6,8], Fugl-Meyer Hand (FMH) [8], The Action Research Arm Test (ARAT) [6,8], The Motor Activity Log [6], time to execute tasks [11], Toronto Rehabilitation Institute Hand Function Test (TRI-HFT) [5], pinch strength [8,10,12], JTFHT [12], Activity of Daily Living (ADL) [13], Functional Independence Measure (FIM) [7], Wolf Motor Function Test (WMFT) [8], Chedoke McMaster Stroke Assessment Hand (CMSAH) [8] and the Quick-DASH [10]. Then, each outcomes measure have been classified according to the International Classification of Functioning, Disability and Health (ICF) [14] (Figure. 1).
Effects and effectiveness
Figure 1. Outcomes measures classified with the CIF, p-values and effect size
The results in terms of effects and effectiveness of the interventions are listed in the Figure 1. Mostly, the use of robotic gloves increased joint mobility and functional capacity of the upper limb in terms of performance rapidity. According to muscular strength, functional capacity of the upper limb assessed by questionnaire, and global functional capacity, the results are heterogeneous and do not allow conclusion on the effectiveness of intervention using this technology.
Usability, feasibility and satisfaction
Four studies also assessed the usability, feasibility or satisfaction of the users after trying the soft robotic glove [10-13] using the Usefulness-Satisfaction-and-Ease-of-Use questionnaire [11], observations [4,10], System Usability Scale [12,13], Intrinsic Motivation Inventory [13], cost analysis [10]. Studies concluded that the use of soft robotic gloves is foreseen as being feasible and acceptable by participants and rehabilitation professionals [10-13] and as increasing engagement in rehabilitation program [11,13]. Most of the studies support the fact that the soft robotic gloves are easy to use [10, 1,13]. However, the robotic glove was found to be more useful when performing gross motor tasks when compared to fine motor tasks [12], the presence of a zipper on the glove made it difficult to put on [13], and the choice of material, especially its thickness, was found to interfere with hand and finger sensations [13]. A preference for the rental of these devices has been demonstrated [11]. The most important features highlighted in the studies included: easy to clean, comfortable, easy to put on and take off. Last, a decreased in rehabilitation cost linked to the use of a soft robotic device at home may be anticipated [10].
DISCUSSION
This systematic review of the literature confirms an increased interest over the last decade in the development and use of soft robotic gloves for rehabilitation of individuals with hand hemiparesis following a neurological event. Overall, the use of soft robotics devices in rehabilitation treatment is feasible, safe, and acceptable by patients while its effects and effectiveness appear promising. However, the strength of the currently available evidence remains limited and given the wide variety of soft robotic glove attributes, study designs and interventions, and outcomes measures alongside the small sample sizes tested, it is impossible to highlight which soft robotic glove or intervention protocol would be the most appropriate to obtain the best clinical results. Stronger evidence linked to the effects or effectiveness, in addition to comprehensive stakeholder perspectives (e.g., patients, rehabilitation professionals), especially on the usability, are needed to ensure a successful transition from the laboratory to clinical practice.
CONCLUSIONS
This systematic review maps currently available evidence on the use of soft robotic gloves as a rehabilitation intervention while considering effectiveness and usability. This technology is a promising solution to optimize sensorimotor capabilities, hand-related functional abilities and facilitate participation in everyday activities while overcoming some clinical constraints. Additional research in this area should be encouraged to strengthen current evidence.
REFERENCES
[1] Chollet, F., DiPiero, V., Wise, R. J. S., Brooks, D. J., Dolan, R. J., & Frackowiak, R. S. J. (1991). The functional anatomy of motor recovery after stroke in humans: a study with positron emission tomography. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society, 29(1), 63-71.
[2] Hubbard, I. J., Parsons, M. W., Neilson, C., & Carey, L. M. (2009). Task‐specific training: evidence for and translation to clinical practice. Occupational therapy international, 16(3‐4), 175-189.
[3] Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal medicine, 151(4), 264-269.
[4]Brokaw, E. B., Black, I., Holley, R. J., & Lum, P. S. (2011). Hand Spring Operated Movement Enhancer (HandSOME): a portable, passive hand exoskeleton for stroke rehabilitation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 19(4), 391-399.
[5] Cappello, L., Meyer, J. T., Galloway, K. C., Peisner, J. D., Granberry, R., Wagner, D. A., … & Walsh, C. J. (2018). Assisting hand function after spinal cord injury with a fabric-based soft robotic glove. Journal of neuroengineering and rehabilitation, 15(1), 59.
[6] Chen, J., Nichols, D., Brokaw, E. B., & Lum, P. S. (2017). Home-based therapy after stroke using the hand spring operated movement enhancer (HandSOME). IEEE Transactions on Neural Systems and Rehabilitation Engineering, 25(12), 2305-2312.
[7] Scott, S., Yu, T., White, T. K., Van Harlinger, W., Ganzalez, Y., Llanos, I., & Kozel, A. F. (2018). A robotic hand device safety study for people with cervical spinal cord injury. Federal practitioner, 35(3), S21-S24.
[8] Thielbar, K. O., Triandafilou, K. M., Fischer, H. C., O’Toole, J. M., Corrigan, M. L., Ochoa, J. M., … & Kamper, D. G. (2017). Benefits of using a voice and EMG-Driven actuated glove to support occupational therapy for stroke survivors. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 25(3), 297-305.
[9] Bernocchi, P., Mulè, C., Vanoglio, F., Taveggia, G., Luisa, A., & Scalvini, S. (2018). Home-based hand rehabilitation with a robotic glove in hemiplegic patients after stroke: a pilot feasibility study. Topics in stroke rehabilitation, 25(2), 114-119.
[10]Vanoglio, F., Bernocchi, P., Mulè, C., Garofali, F., Mora, C., Taveggia, G., … Luisa, A. (2017). Feasibility and efficacy of a robotic device for hand rehabilitation in hemiplegic stroke patients: a randomized pilot-controlled study. Clinical rehabilitation, 31(3), 351-360.
[11] Yap, H. K., Lim, J. H., Nasrallah, F., & Yeow, C. H. (2017). Design and preliminary feasibility study of a soft robotic glove for hand function assistance in stroke survivors. Frontiers in neuroscience, 11, 547.
[12] Prange-Lasonder, G. B., Radder, B., Kottink, A. I., Melendez-Calderon, A., Buurke, J. H., & Rietman, J. S. (2017, July). Applying a soft-robotic glove as assistive device and training tool with games to support hand function after stroke: Preliminary results on feasibility and potential clinical impact. In Rehabilitation Robotics (ICORR), 2017 International Conference on (pp. 1401-1406). IEEE.
[13] Radder, B., Prange-Lasonder, G. B., Kottink, A. I., Melendez-Calderon, A., Buurke, J. H., & Rietman, J. S. (2018). Feasibility of a wearable soft-robotic glove to support impaired hand function in stroke patients. Journal of rehabilitation medicine, 50(7), 598-606.
[14] World Health Organization. (2001). International classification of functioning, disability and health: ICF. Geneva: World Health Organization.
ACKNOWLEDGMENTS
Supported by the Initiative for the Development of New Technologies and Innovative Practices in Rehabilitation and by the Université de Montréal (Direction des affaires internationales).
In the present work, we investigated the relationship of oscillatory sensorimotor brain activity to motor recovery. The neurophysiological data of 30 chronic stroke patients with severe upper‐limb paralysis are the basis of the observational study presented here. These patients underwent an intervention including movement training based on combined brain–machine interfaces and physiotherapy of several weeks recorded in a double‐blinded randomized clinical trial. We analyzed the alpha oscillations over the motor cortex of 22 of these patients employing multilevel linear predictive modeling. We identified a significant correlation between the evolution of the alpha desynchronization during rehabilitative intervention and clinical improvement. Moreover, we observed that the initial alpha desynchronization conditions its modulation during intervention: Patients showing a strong alpha desynchronization at the beginning of the training improved if they increased their alpha desynchronization. Patients showing a small alpha desynchronization at initial training stages improved if they decreased it further on both hemispheres. In all patients, a progressive shift of desynchronization toward the ipsilesional hemisphere correlates significantly with clinical improvement regardless of lesion location. The results indicate that initial alpha desynchronization might be key for stratification of patients undergoing BMI interventions and that its interhemispheric balance plays an important role in motor recovery.
1 INTRODUCTION
Stroke is a major global health problem. The number of stroke victims has been rising in the past years all around the world. Millions of stroke survivors are left with very limited motor function or complete paralysis and depend on assistance (Feigin et al., 2016). Therapeutic approaches such as constraint‐induced movement therapy are not applicable to the group of patients with severe limb weakness (Birbaumer, Ramos‐Murguialday, & Cohen, 2008). However, brain–machine interface (BMI) training has demonstrated efficacy in promoting motor recovery in chronic paralyzed stroke patients (Ramos‐Murguialday et al., 2013), and long term effects (Ramos‐Murguialday et al., 2019). Subsequent work has replicated and confirmed BMI efficacy. Arm and hand movements are trained using a body actuator (e.g., orthotic robots) that is controlled by oscillatory activity of the brain (Ang et al., 2014; Frolov et al., 2017; Kim, Kim, & Lee, 2016; Leeb et al., 2016; Mokienko et al., 2016; Ono et al., 2014). Brain signals can thus travel to the limb muscles along an alternative pathway. Contingently linking movement‐related patterns of brain activity and visuo‐proprioceptive feedback of the movement supports associative learning (Ramos‐Murguialday et al., 2012; Sirigu et al., 1995).
Changes in sensorimotor brain oscillations involved in planning and execution of movements were used as control signals for the BMI in the aforementioned studies. The sensorimotor rhythm (SMR) is an oscillation within the alpha frequency range of the EEG during a motionless resting state over the central‐parietal brain regions. Movement planning, imagination and execution lead to its suppression. In the present work, we investigate EEG brain oscillations of the alpha frequency, ranging from 8 to 12 Hz, over the motor cortex, and we term them “alpha oscillations.”
Biomarkers could be defined as indicators “of disease state that can be used as a measure of underlying molecular/cellular processes that may be difficult to measure directly in humans” (Boyd et al., 2017). When dealing with a condition as heterogeneous as stroke validated biomarkers of recovery could help plan treatments and support efficient allocation of resource while maximizing outcome for the patients. Alpha brain oscillations have been evaluated as markers of ischaemia and predictors of clinical outcome in acute patients (Finnigan & van Putten, 2013; Rabiller, He, Nishijima, Wong, & Liu, 2015). Desynchronization in the alpha frequency range has also been investigated as a marker of stroke and a predictor of recovery in the same patient group. Tangwiriyasakul, Verhagen, Rutten, and Putten (2014) showed that the recovery of motor function was accompanied by an increase of alpha desynchronization on the ipsilesional side. In subacute patients presenting mild to moderate motor deficits recovery lead to a similar increase of alpha desynchronization on the affected hemisphere (Platz, Kim, Engel, Kieselbach, & Mauritz, 2002). Furthermore, first attempts investigated correlations of alpha desynchronization with motor improvements in chronically impaired patients (Kaiser et al., 2012). In a controlled study, a group of subacute patients with severe deficits used motor imagery, guided by a brain–computer interface, in addition to their regular physiotherapeutic rehabilitation protocol. They showed a higher probability for motor improvements with increased alpha desynchronization (Pichiorri et al., 2015).
In the present work, we investigated what changes in the oscillatory activity of the brain a proprioceptive BMI coupled with physiotherapy produces over the course of a training intervention and if these correlate with recovery in severely paralyzed chronic stroke patients. We hypothesized that functional motor improvements are accompanied by an ipsilesional increase and a contralesional decrease in alpha desynchronization indicating reorganization of compensatory brain activity from the contralesional to the ipsilesional hemisphere. We intend to establish alpha oscillatory activity as a biomarker of motor impairment and as a building block of statistical models of stroke neurorehabilitation.[…]
Figure 1 Schematics of the data acquisition phase and the offline analysis for EEG and EMG. Neurophysiological data was acquired using a 16 channel EEG cap and 4 bipolar EMG electrodes on each arm. EEG data were cleaned from eye movement artifacts and trials containing other artifacts (e.g., cranial EMG, head movements, and so on). EMG data were analyzed to detect compensatory muscle contractions on the healthy upper limb and on the paretic side during resting intervals to identify these trials as contaminated because the muscle activity is a sign of undesired EEG activity. Only data free of artifacts were used for the final analysis of EEG oscillatory activity
Background and Purpose: Current literature has focused on identifying neuroplastic changes associated with stroke through tasks and in positions that are not representative of functional rehabilitation. Emerging technologies such as functional near-infrared spectroscopy (fNIRS) provide new methods of expanding the area of neuroplasticity within rehabilitation. This study determined the differences in sensorimotor cortex activation during unrestrained reaching and gripping after stroke.
Methods: Eleven individuals with chronic stroke and 11 neurologically healthy individuals completed reaching and gripping tasks under 3 conditions using their (1) stronger, (2) weaker, and (3) both arms together. Performance and sensorimotor cortex activation using fNIRS were collected. Group and arm differences were calculated using mixed analysis of covariance (covariate: age). Pairwise comparisons were used for post hoc analyses. Partial Pearson correlations between performance and activation were assessed for each task, group, and hemisphere.
Results: Larger sensorimotor activations in the ipsilesional hemisphere were found for the stroke compared with healthy group for reaching and gripping conditions despite poorer performance. Significant correlations were observed between gripping performance (with the weaker arm and both arms simultaneously) and sensorimotor activation for the stroke group only.
Discussion and Conclusions: Stroke leads to significantly larger sensorimotor activation during functional reaching and gripping despite poorer performance. This may indicate an increased sense of effort, decreased efficiency, or increased difficulty after stroke. fNIRS can be used for assessing differences in brain activation during movements in functional positions after stroke. This can be a promising tool for investigating possible neuroplastic changes associated with functional rehabilitation interventions in the stroke population.
Video Abstract available for more insights from the authors (see Video Abstract, Supplemental Digital Content 1, available at: http://links.lww.com/JNPT/A269).
INTRODUCTION
Stroke is the leading cause of long-term disability in Canada, with approximately 405 000 Canadians currently living with its long-lasting effects.1 While the site of injury and the specific presentation of symptoms are heterogeneous, up to 70% of these individuals experience upper extremity hemiparesis,2 and even after rehabilitation, greater than 65% of this population have difficulty utilizing their affected limb in activities of daily living.3 Decreased use of the paretic arm can lead to chronic pain and weakness, decreased bone density,4 cerebral cortex changes,5and an overall decrease in quality of life.6 In addition, stroke rehabilitation and continual care are costly for the health care system.7 Therefore, it is important to maximize patient recovery in an effective and efficient manner.
One area that has been highly debated for rehabilitation efficacy is the side of arm training. Numerous reviews have stated conflicting and inconclusive results pertaining to benefits of the paretic (affected) arm or bilateral arm training8–10 and a few studies have recently investigated the effects of the nonparetic (less-affected) arm training.11,12 Investigating how stroke itself affects neural activation during unilateral and bilateral upper extremity activities may help explain the mechanisms underlying such training.
In individuals living with the chronic effects of stroke, nonnormal brain activation is commonly seen with irregular activation in both the ipsi- and contralesional hemispheres during movement. A meta-analysis of 20 studies13 calculated increases in contralesional primary motor cortex, and bilateral premotor and supplementary motor areas with use of the paretic hand compared with healthy individuals. Systematically reviewing 22 functional magnetic resonance imaging (fMRI) and positron emission tomography studies, Buma et al14 reported general initial increases in contra-, ipsi-, and perilesional activation during paretic upper extremity movement in individuals with cortical and subcortical strokes when compared with healthy adults. In addition, as paretic arm performance increased with training, these authors also showed that in many, but not all participants, activation decreased in areas such as the contralesional motor cortex (ie, ipsilateral to the movement arm), which is not typically activated in healthy individuals. Previous reviews have also reported increases in cortical activation of motor supporting areas (bilateral premotor and supplementary motor areas) later in recovery that are associated with greater function,15 although the opposite has also been reported.16
The majority of previously mentioned evidence utilized neuroimaging techniques that require an individual to remain fairly still, especially at the head, and recorded in the supine position. While there are many advantages to these techniques, such as high spatial resolution and penetration depth using fMRI, the functional imaging data acquired from these studies may not be truly indicative of the neural correlates involved during rehabilitation tasks. Thus, assessment of brain activation during upright, unrestrained, functional tasks is needed. Functional near-infrared spectroscopy (fNIRS) is an emerging neuroimaging device that has the capabilities of determining cortical activation while the participant is mobile. Similar to fMRI, fNIRS is an indirect measure of cortical activation that utilizes the neurovascular coupling theory to estimate changes in brain activity.17 Near-infrared light emitted by this device is absorbed by areas high in oxyhemoglobin or deoxyhemoglobin content and is measured through detectors placed on the individual’s head. When an increase in brain activity occurs, a typical overall increase in oxyhemoglobin concentration and a slight decrease in deoxyhemoglobin are observed.17 Due to its portability, fNIRS has been used to investigate cortical activation during various mobile tasks after stroke.18,19 To our knowledge, no work has been done to compare sensorimotor cortex activation of paretic, nonparetic, and bilateral arm movements poststroke using fNIRS.
Therefore, the primary purpose of this study was to investigate differences in cortical brain activation during performance of upper extremity activities in an upright position after stroke and in neurologically healthy individuals. Based on the current evidence, we hypothesized that greater sensorimotor cortex activation would be observed in the stroke group compared with the neurologically healthy group, particularly when using the weaker arm. For our secondary measures, we hypothesize that (1) individuals in the stroke group will perform worse than the control group when using their weaker arm and (2) cortical activation in the contralateral hemisphere (eg, ipsilesional hemisphere during paretic arm movements) will positively correlate with task performance.[…]
Figure 1 (A) Schematic of the environmental setup for the reaching task. Two adjacent Box and Block sets were placed in front of the participant. The left box was for the left hand and the right box was for the right hand. Arrows indicate the movement of the blocks from the box closest to the participant to the box further in front of the participant. (B) Schematic of the optode placements with reference to the international 10/10 system. Source probes are indicated by black circles and detector probes are indicated by gray circles. Source Increased Sensorimotor Cortex Activation With Decreased Motor Performance During Functional Upper Extremity Tasks Poststroke Journal of Neurologic Physical Therapy43(3):141-150, July 2019.
Purpose: To evaluate the effectiveness of the Bobath concept in sensorimotor rehabilitation after stroke.
Materials and methods: A systematic literature review was conducted on the Bobath concept from the first publication available to January 2018, consulting PUBMED, CENTRAL, CINAHL and PEDro databases. Fifteen clinical trials were selected in two consecutive screenings. Two independent researchers rated the studies according to the PEDro scale from which a best evidence synthesis was derived to determine the strength of the evidence.
Results: The Bobath concept is not more effective than other approaches used in post-stroke rehabilitation. There is moderate evidence for the superiority of other therapeutic approaches such as forced use of the affected upper limb and constraint-induced movement therapy for motor control of the upper limb.
Conclusions: The Bobath concept is not superior to other approaches for regaining mobility, motor control of the lower limb and gait, balance and activities of daily living of patients after stroke. There is moderate evidence regarding the superior results of other approaches in terms of the motor control and dexterity of the upper limb. Due to the limitations concerning the methodological quality of the studies, further well-designed studies are needed.
Implications for rehabilitation
The Bobath concept is not superior to other approaches for patients after stroke.
The treatments that incorporate overuse of the affected upper limb via intensive treatments with high-repetitions with or without robotic aids present greater effectiveness in the motor control of the upper limb and dexterity.
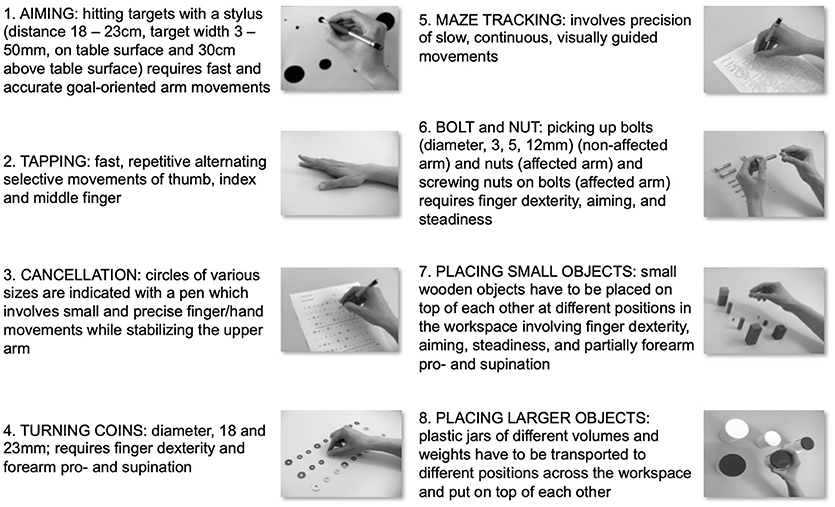
Arm Ability Training (AAT) has been specifically designed to promote manual dexterity recovery for stroke patients who have mild to moderate arm paresis. The motor control problems that these patients suffer from relate to a lack of efficiency in terms of the sensorimotor integration needed for dexterity. Various sensorimotor arm and hand abilities such as speed of selective movements, the capacity to make precise goal-directed arm movements, coordinated visually guided movements, steadiness, and finger dexterity all contribute to our “dexterity” in daily life. All these abilities are deficient in stroke patients who have mild to moderate paresis causing focal disability. The AAT explicitly and repetitively trains all these sensorimotor abilities at the individual’s performance limit with eight different tasks; it further implements various task difficulty levels and integrates augmented feedback in the form of intermittent knowledge of results. The evidence from two randomized controlled trials indicates the clinical effectiveness of the AAT with regard to the promotion of “dexterity” recovery and the reduction of focal disability in stroke patients with mild to moderate arm paresis. In addition, the effects have been shown to be superior to time-equivalent “best conventional therapy.” Further, studies in healthy subjects showed that the AAT induced substantial sensorimotor learning. The observed learning dynamics indicate that different underlying sensorimotor arm and hand abilities are trained. Capacities strengthened by the training can, in part, be used by both arms. Non-invasive brain stimulation experiments and functional magnetic resonance imaging data documented that at an early stage in the training cortical sensorimotor network areas are involved in learning induced by the AAT, yet differentially for the tasks trained. With prolonged training over 2 to 3 weeks, subcortical structures seem to take over. While behavioral similarities in training responses have been observed in healthy volunteers and patients, training-induced functional re-organization in survivors of a subcortical stroke uniquely involved the ipsilesional premotor cortex as an adaptive recruitment of this secondary motor area. Thus, training-induced plasticity in healthy and brain-damaged subjects are not necessarily the same.
Motor Deficits of Stroke Survivors With Mild to Moderate Arm Paresis
Arm paresis post stroke shows a bi-modal distribution. Many stroke survivors have either severe arm paresis and are only able to use their arms functionally in everyday life to a very limited extent, if at all, or mild to moderate arm paresis with the ability to use their paretic arm for functional tasks, yet with a lack of dexterity (1, 2). Thus, the motor control deficits of these subgroups are quite different and hence so too are their therapeutic needs.
Clinically, stroke survivors with mild to moderate arm paresis have reduced strength and endurance of their paretic arm and are functionally limited by a lack of speed, accuracy and co-ordination of arm, hand, and finger movements and a lack of dexterity when handling objects. Key to understanding any functional deficits and the need and opportunities to improve function by training is a focused analysis of the specific motor control deficits involved in this clinical syndrome. A way to do this is to test various domains of sensorimotor control that have been shown to be independent by factorial analysis (3, 4).
When motor performance of healthy people across various tasks has been analyzed by factorial analysis certain independent arm motor abilities have been documented. These are different independent sensorimotor capacities that together contribute to our skilfulness in everyday life. What are these abilities? They are our ability to make fast selective wrist and finger movements (wrist-finger speed), to manipulate small objects (finger dexterity) or larger objects (manual dexterity) efficiently, our ability to keep our arm steady (steadiness), to move our arm quickly and precisely to an intended target (aiming), or to move it under constant visual control along a line (tracking) (5).
When tested among stroke survivors with mild to moderate arm paresis all these abilities are deficient, indicating the complex nature of sensorimotor control deficits in this clinical condition (6, 7).
The Arm Ability Training as a “Tailor-Made training” to Meet Specific Rehabilitation Demands
The Arm Ability Training (AAT) was designed to train all these sensorimotor abilities and thus to meet the specific rehabilitation demands of this subgroup of stroke survivors (8, 9). The eight training tasks collectively cover these affordances (Figure 1).
Figure 1. Training tasks of the Arm Ability Training. Description of the eight training tasks of the Arm Ability Training (AAT) that are repetitively exercised daily. Together they train various independent arm and hand sensorimotor abilities. During the AAT sensorimotor performance is trained at its individual limit. Further aspects thought to promote motor learning are a high repetition rate of trained tasks, variation in the difficulty of training tasks, and the augmented feedback provided in the form of intermittent knowledge of the results.
Recent evidence suggests that impaired central sensorimotor integration may contribute to deficits in movement control experienced by people with chronic ankle instability (CAI). This study compared the effects of dual-task and walking speed on gait variability in individuals with and without CAI.
Methods
Sixteen subjects with CAI and 16 age- and gender-matched, able-bodied controls participated in this study. Stride time variability and stride length variability were measured on a treadmill under four different conditions: self-paced walking, self-paced walking with dual-task, fast walking, and fast walking with dual-task.
Results
Under self-paced walking (without dual-task) there was no difference in stride time variability between CAI and control groups (P = 0.346). In the control group, compared to self-paced walking, stride time variability decreased in all conditions: self-paced walking with dual-task, fast speed, and fast speed with dual-task (P = 0.011, P = 0.016, P = 0.001, respectively). However, in the CAI group, compared to self-paced walking, decreased stride time variability was demonstrated only in the fast speed with dual-task condition (P = 1.000, P = 0.471, P = 0.008; respectively). Stride length variability did not change under any condition in either group.
Conclusions
Subjects with CAI and healthy controls reduced their stride time variability in response to challenging walking conditions; however, the pattern of change was different. A higher level of gait disturbance was required to cause a change in walking in the CAI group compared to healthy individuals, which may indicate lower adaptability of the sensorimotor system. Clinicians may use this information and employ activities to enhance sensorimotor control during gait, when designing intervention programs for people with CAI.
The study was registered with the Clinical Trials network (registration NCT02745834, registration date 15/3/2016).
Background
Recurrent ankle sprains occur in up to 40% of individuals who have previously experienced a lateral ankle sprain [1, 2]. Individuals who report residual symptoms, which include repetitive episodes of ‘giving way’ and subjective feeling of ankle joint instability are termed as having chronic ankle instability (CAI) [3]. The cause of these symptoms and the high frequency of recurrent ankle sprain is not fully understood [4]. It has been suggested that the residual joint instability and the high reoccurrence rates can be attributed to loss of sensory input from articular mechano-receptors, decreased muscle strength, mechanical instability of the ankle joint, and reduced ankle range of motion [5, 6].
Recent evidence suggests that deficits in central neural sensorimotor integration can contribute to impaired movement control in people with CAI [7, 8, 9, 10, 11, 12, 13, 14]. For example, Springer et al. [8] assessed the correlation between single-limb stance postural control (Overall Stability Index) and shoulder position sense (Absolute Error Score) among people with CAI and healthy controls. Correlations between the lower and upper limbs were observed only in the healthy controls, indicating altered sensorimotor integration in the CAI group. Several studies have observed altered gait mechanism in people with CAI, which was explained by compromised central nervous system (CNS) control [9, 14, 15, 16]. It was shown that people with CAI have a typical gait pattern of increased inversion kinematics and kinetics, lateral shift of body weight, increased hip flexion during terminal swing to mid stance, reduced hip extension and increased knee flexion during terminal stance to initial swing, and slow weight transfer at the beginning and end of the stance [15, 16, 17]. Altered biomechanical strategies during gait initiation and termination tasks (e.g., reduced center of pressure displacement), have also been demonstrated in this population [9, 14]. Studies that assessed movement variability, such as knee and hip joint motions during single leg jump landing, identified differences between individuals with and without CAI, which may also indicate central motor programming deficits [10, 11, 12, 13]. Hence, further investigation of motor control adaptations may contribute to understanding the underlying neurophysiologic mechanisms of CAI.
Gait speed and other spatio-temporal parameters during daily activities should reflect behavioral goals and environmental conditions [18]. Studies revealed that walking speed has a significant effect on joint coordination pattern and gait variability [18, 19, 20]. Therefore, assessing gait variability under challenging situations such as walking at different speeds might test CNS flexibility in controlling gait [19, 20]. Moreover, based on the understanding that for many daily activities even a fully intact motor control system requires attention and cognitive resources [21], the dual-task paradigm has been used to provide insight into the demands of postural control and gait on attention. Performance of a cognitive task has been shown to decrease postural control in participants with CAI as compared to healthy controls [7, 22]. However, no previous study examined the impact of cognitive task and walking speed on gait performance in subjects with CAI.
Balance during walking is reflected by precise spatial and temporal control of foot placement. Stride to stride fluctuations in time and length are related to control of the rhythmic walking mechanism. Thus, previous research has suggested that studying gait variability is a reliable way to quantify locomotion [23]. The mechanism of adjusting movement variability is considered beneficial for coping with changes, maintaining stability, preventing injury, and attaining higher motor skills [24]. Performing a cognitive task while walking or while altering self-paced walking speed has been related to changes in gait variability in populations with neurological and musculoskeletal pathologies, as well in healthy young individuals [25, 26, 27, 28]. Yet, there is no consensus in the literature as to how to interpret these changes. Decreased variability while performing demanding gait tasks may reflect voluntary gait adaptation toward a more conservative gait pattern [26]. Alternatively, it has been suggested that increased variability may indicate CNS flexibility and adaptability to changes in task demands [29]. A possible central sensorimotor control deficit in people with CAI may constrain the ability of the CNS to adjust to different task demands; thus, affecting central control over gait variability and reducing the ability to cope with varied tasks. Consequently, testing the mechanism of adjusting gait variability as a response to complex walking conditions in people with CAI compared to healthy controls may provide more information on sensorimotor control in this population.
The present study was designed to compare the effects of dual-task and walking speed on gait variability in individuals with and without CAI. Previous reports, including a meta-analysis, indicated that simple postural tasks do not always discriminate between participants with CAI and those without [6, 8, 30]. Consequently, we hypothesized that gait variability among individuals with and without CAI will be similar during “normal” self-paced walking, whereas gait will vary under complex walking conditions.[…]
Finding, testing and demonstrating efficacy of new treatments for stroke recovery is a multifaceted challenge. We believe that to advance the field, neurorehabilitation trials need a conceptually rigorous starting framework. An essential first step is to agree on definitions of sensorimotor recovery and on measures consistent with these definitions. Such standardization would allow pooling of participant data across studies and institutions aiding meta-analyses of completed trials, more detailed exploration of recovery profiles of our patients and the generation of new hypotheses. Here, we present the results of a consensus meeting about measurement standards and patient characteristics that we suggest should be collected in all future stroke recovery trials. Recommendations are made considering time post stroke and are aligned with the international classification of functioning and disability. A strong case is made for addition of kinematic and kinetic movement quantification. Further work is being undertaken by our group to form consensus on clinical predictors and pre-stroke clinical data that should be collected, as well as recommendations for additional outcome measurement tools. To improve stroke recovery trials, we urge the research community to consider adopting our recommendations in their trial design.
Introduction
Lack of a standardized approach to measurement in stroke recovery research hampers our ability to advance understanding of recovery mechanisms, devise better treatments and consolidate knowledge from a body of research using meta-analyses.1 As examples, examination of a recent Cochrane Overview of interventions to improve upper limb function after stroke identified 208 unique assessment tools from 243 trials2; another review found more than 100 measures of activities of daily living (ADLs).3 Furthermore, in most motor rehabilitation trials, measures are taken at arbitrary time points relative to stroke onset, e.g. time of admission to, or discharge from, rehabilitation rather than at standard time points aligned with underlying recovery processes.4
We must challenge the common assumption that most sensorimotor therapies are universally applicable and will achieve the same benefit for all people with stroke. The magnitude of change and likelihood of achieving clinically meaningful improvement in response to specific therapies will depend on age, stroke severity, and other factors including pre-existing comorbid conditions (e.g. diabetes, cognitive impairment, depression)5 and pre-stroke lifestyle factors (e.g. social engagement, exercise).6 The respective contributions of these factors have yet to be fully understood. Going forward, we need to identify the determinants that may help predict responders and non-responders to interventions.
The measurement working group of the Stroke Recovery and Rehabilitation Roundtable (SRRR)7 was established to develop recommendations for standardized assessment time points and measures to be included in all adult trials of sensorimotor recovery after stroke. Given the current lack of standards for data collection and heterogeneous reports in stroke recovery trials, our expert group also considered pre-stroke clinical, demographic and stroke-related data that should be collected to improve clinical prediction of recovery and characterization of patient cohorts.
The decision to focus on sensorimotor recovery reflects the volume of existing trials in this area, the range of outcomes currently in use across these trials, and the gap in current research that known international initiatives has not addressed (e.g. Core Outcome Measures in Effectiveness Trials Initiative (COMET), National Institute of Neurological Disorders and Stroke Common Data Elements (NINDS CDE), The International Consortium for Health Outcomes Measurement (ICHOM),8 Improving Research Outcome Measurement in Aphasia (ROMA)9 and Standardization of Measures in Arm Rehabilitation Trials after Stroke (SMART), Supplementary Table 1). Acknowledging that clinical measures cannot distinguish between true neurological repair (behavioral restitution) and use of compensatory strategies,10 a second objective was to consider whether we could recommend specific kinetic and/or kinematic outcomes that reflect quality of motor performance in order to better understand the neurophysiological changes that occur when patients improve.11,12 Our overall objective of the roundtable was to provide recommendations that, if applied, could improve the methodology of rehabilitation and recovery trials, help build our understanding of the trajectory of stroke recovery and aid discovery of new and more targeted treatments.